When most parents think of sleep apnea, they picture loud, disruptive snoring. But in many children, obstructive sleep apnea (OSA) doesn’t sound like much at all.
That’s where the term silent apnea comes in when a child stops breathing during sleep but shows no obvious snoring. It’s easy to overlook, but the risks are just as real.
What Is Silent Apnea in Children?
Silent apnea refers to episodes of airway blockage without the hallmark sound of snoring. This can occur when the child’s throat muscles relax too much during sleep, partially or completely closing the airway.
Because kids have more flexible airways and smaller necks, obstructions can happen without causing the vibration that makes snoring noises.
Instead, breathing pauses may be completely quiet sometimes lasting 10 seconds or more making it easy for even attentive parents to miss.
Why Don’t All Children Snore?
There are a few reasons why snoring may be absent, even with confirmed apnea:
- Anatomy: Children with high-arched palates, recessed jaws, or nasal obstruction may breathe silently, even during pauses.
- Sleep position: Back sleeping can trigger apnea without snoring in some kids.
- Muscle tone: In certain cases, children with low muscle tone (e.g., from neuromuscular conditions) don’t generate enough vibration to produce sound.
- Age: Younger children, especially toddlers, may not have developed the same airway dynamics that cause snoring in adults.
This makes it crucial to look for non-auditory clues if you suspect something is off with your child’s sleep.
Signs of Silent Apnea in Children
Even without snoring, silent apnea may cause subtle but impactful symptoms:
Nighttime Symptoms
- Pauses in breathing (watch the chest)
- Mouth breathing
- Tossing and turning
- Night sweating
- Restlessness
- Bedwetting (especially after age 5)
Daytime Symptoms
- Morning headaches
- Difficulty waking up
- Fatigue despite full sleep hours
- Poor focus in school
- Irritability or hyperactivity
- Slower growth or weight gain
One red flag: if your child consistently wakes up more tired than before bed, or shows behavioral issues during the day, apnea should be ruled out even if snoring isn’t present.
You can see more signs listed in this Stanford Children’s Health overview.
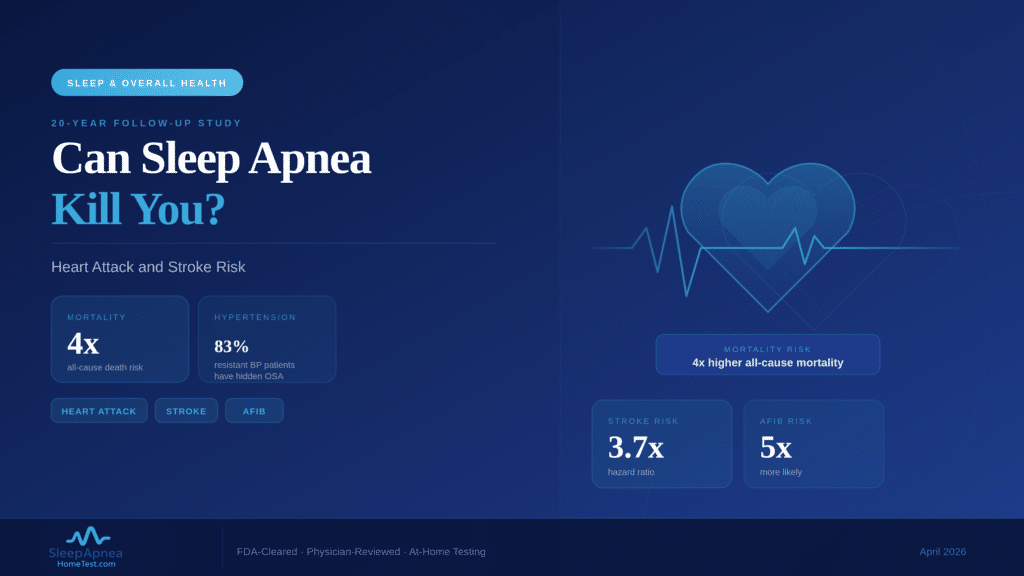
Is Silent Apnea Dangerous?
Yes. Untreated OSA silent or not can have long-term effects on a child’s:
- Cognitive development
- Behavior and mood
- Heart health
- Immune system
- Growth hormone release (which primarily occurs during deep sleep)
Children with untreated OSA are at higher risk for ADHD-like behavior, poor school performance, and even cardiovascular stress. That’s why early diagnosis matters.
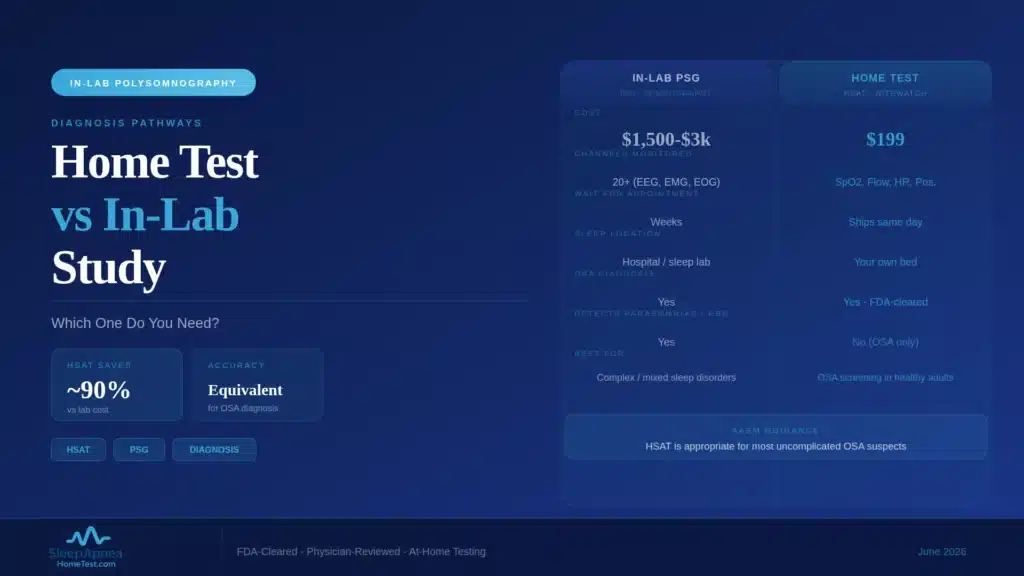
How Is Silent Apnea Diagnosed Without Snoring?
Diagnosis relies on objective sleep data not sound alone. Your pediatrician may refer your child for:
-
Overnight Sleep Study (Polysomnography)
The gold standard for diagnosis, this test measures:
- Brain waves
- Oxygen levels
- Breathing effort
- Airflow
- Chest movement
- Sleep stages
It picks up apneas, hypopneas, and oxygen drops whether the child snores or not.
-
Home Sleep Testing (Case-by-Case)
While in-lab studies are ideal for kids, home testing may be considered for teens or under specific clinical guidance.
Talk to your doctor about the best option based on age, symptoms, and comorbidities.
What Causes Silent Apnea in Kids?
Common triggers include:
- Enlarged tonsils/adenoids (most frequent cause in ages 2–7)
- Craniofacial differences (e.g., narrow jaw, recessed chin)
- Allergic rhinitis or nasal blockage
- Obesity (especially in older children)
- Neuromuscular tone issues
- Premature birth history
Sometimes, no single factor is found just a combination of airway structure and sleep muscle relaxation.
What Are the Treatment Options?
Treatment depends on the severity and root cause. Your ENT or pediatric sleep specialist may recommend:
- Adenotonsillectomy (removal of tonsils/adenoids)
- Nasal sprays or allergy control
- Orthodontic interventions (like palate expanders)
- Weight management if obesity is a factor
- CPAP or BiPAP for moderate to severe cases
In some children, especially those with underlying conditions, long-term airway support during sleep is needed even if snoring is never present.
How to Monitor at Home
Until formal testing is done, consider:
- Video recording sleep (audio may miss episodes)
- Keeping a symptom journal: note morning behavior, mood, and nighttime restlessness
- Watching for mouth breathing and gasping
You can also try validated pediatric screeners like the Pediatric Sleep Questionnaire (PSQ) and discuss results with your pediatrician.
Why Awareness Matters
Because silent apnea doesn’t sound like the adult version, many children go years without diagnosis. They’re labeled as:
- “Restless sleepers”
- “Difficult in class”
- “Not morning people”
…when in fact, interrupted oxygen during sleep may be at the root.
The good news? Once identified, childhood apnea is highly treatable and most children show dramatic improvements in energy, focus, growth, and mood after care begins.
Conclusion: Don’t Rely on Snoring Alone
If your child breathes quietly at night but still shows signs of poor sleep or daytime fatigue, don’t dismiss the possibility of apnea. Silent cases are real, and just as important to diagnose.
Talk to your pediatrician about a referral for a sleep study snoring is optional, but oxygen is not.