Sleepwalking, medically known as somnambulism, belongs to a family of nighttime behaviors called parasomnias. While most episodes last only a few minutes, a wrong turn near stairs or a street can spell trouble. Below you’ll find what drives sleepwalking, why it’s risky, and the best ways to prevent midnight mishaps.
What Happens During Sleepwalking?
Unlike REM sleep, when muscles go limp, sleepwalking strikes during deep non‑REM stages. Electrical signals in the brain get stuck between sleeping and waking, allowing large muscle groups to activate while consciousness stays dim. Polysomnography confirms bursts of delta waves overlapping with lighter stage‑2 patterns, details outlined in this parasomnia overview.
Common Causes and Triggers
| Trigger | How It Sets Off Somnambulism |
| Sleep deprivation | Deepens slow‑wave sleep, boosting arousal confusion. |
| Stress or anxiety | Raises nighttime cortisol, fragmenting deep sleep. |
| Fever or illness | Alters brain temperature regulation, promoting arousals. |
| Certain medications (e.g., zolpidem, beta‑blockers) | Shift sleep architecture toward unstable stages, as shown in this drug‑related parasomnia study. |
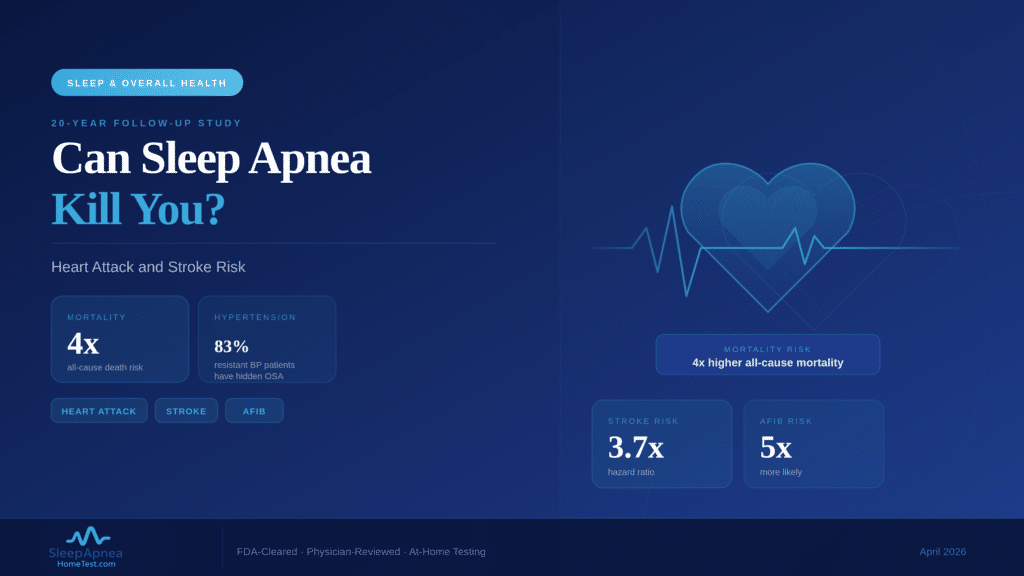
| Obstructive sleep apnea | Repeated breathing pauses trigger micro‑arousals that spill into motor activity. |
| Genetics | First‑degree relatives carry up to a ten‑fold higher risk, per a family linkage analysis. |
Children sleepwalk more because they log more deep sleep and have developing nervous systems; most outgrow it by the teen years.
Risks and Dangers Associated with Sleepwalking
- Household accidents: Falls down stairs or bumping into furniture are common ER stories.
- Outdoor exposure: Front doors can unlock if the wanderer knows the latch well enough while awake.
- Cooking injuries: Cases of sleep‑cooking have led to burns and house fires.
- Violent behavior: Rare but documented in forensic sleep medicine; confusion reactions can mimic aggression. A legal review in Sleep Medicine Reviews discusses sleep‑related violence.
Diagnosing Sleepwalking vs. Other Disorders
- Detailed history – Ask bed partners about timing, behaviors, and possible triggers.
- Sleep diary or wearable data – Track bedtime, wake‑ups, and exercise for two weeks.
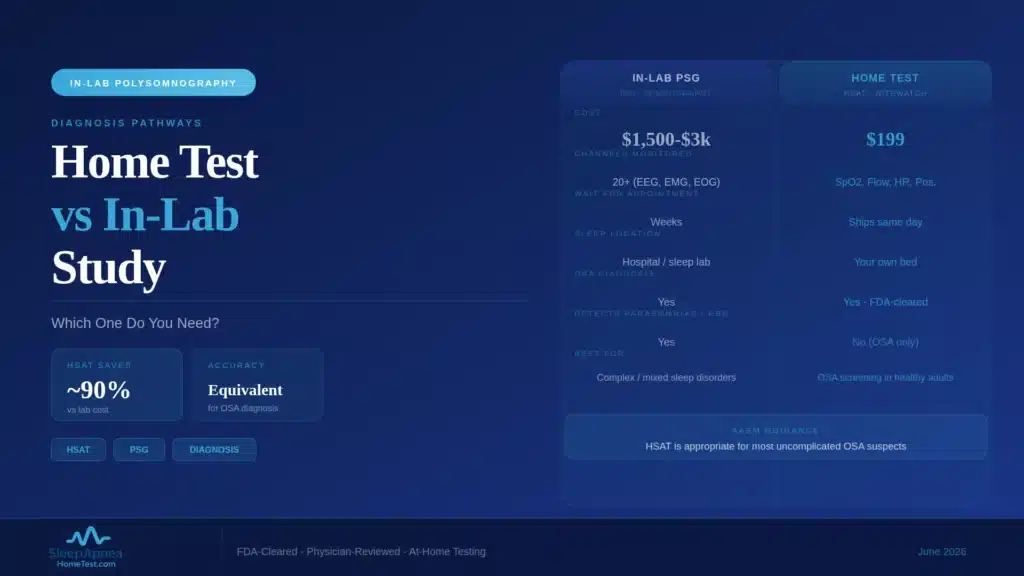
- Overnight sleep study – Needed if snoring, choking, or limb jerks suggest another disorder.
- AI facial scan – Our 60‑second risk screen spots craniofacial traits linked to sleep apnea, a frequent co‑trigger for parasomnias.
Practical Prevention Strategies
Optimize Sleep Schedule
Aim for 7–9 hours nightly. Consistent sleep and wake times stabilize deep‑sleep pressure. Guidance from the American Academy of Sleep Medicine underscores schedule regularity as a first‑line defense.
Cool, Safe Bedroom Design
- Keep the room 18 °C–20 °C; cooler temps reduce arousal frequency.
- Install child‑proof latches on windows and exterior doors.
- Remove tripping hazards and secure stair gates if needed.
Limit Evening Triggers
- Skip heavy meals or alcohol within three hours of bed; both fragment deep sleep, according to this nutrition‑sleep study.
- Hold off on screen time 60 minutes before lights‑out; blue light delays melatonin.
Stress‑Taming Wind‑Down Routine
Five minutes of diaphragmatic breathing inhale 4, hold 4, exhale 6 lowers sympathetic tone. The relaxation response outlined by Harvard Health shows heart rate drops within two minutes.
Medical and Behavioral Treatments
| Option | When to Use | Evidence |
| Scheduled awakenings | Kids with clustered episodes | Reduces frequency by 70 % after two weeks (pediatric trial in Pediatrics). |
| Low‑dose clonazepam | Adults with injury‑risk episodes | Short‑term use lowers event count; monitor next‑day drowsiness. |
| Cognitive Behavioral Therapy (CBT) | Stress or PTSD triggers | CBT targets hyperarousal; see protocol via the CBT‑I toolkit. |
| CPAP or oral appliance | Coexisting OSA | Clearing airway cuts micro‑arousals driving sleepwalking. |
Always consult a sleep specialist before starting medication; wrong doses can worsen confusion arousals.
Safety Checklist for Bed Partners
- Keep car keys out of reach.
- Place a motion sensor near bedroom doors.
- Use a low night‑light in hallways for gentle visibility.
- Discuss a calm redirection script never shout or shake the sleepwalker; guide them gently back to bed.
When to Seek Professional Help
- Episodes result in injury or near‑misses.
- Behavioral strategies fail after one month.
- Snoring, gasping, or restless limb movements accompany the episodes.
- Daytime sleepiness or memory gaps escalate.
A board‑certified sleep physician can tailor a plan that addresses both neurological triggers and environmental safety.
Key Takeaways
- Sleepwalking springs from deep non‑REM sleep when brain signals partially wake muscles but not awareness.
- Sleep loss, stress, certain drugs, and untreated sleep apnea are leading triggers.
- Home safety locks, gates, motion sensors prevents injuries.
- Regular schedules, cool bedrooms, and brief relaxation drills lower episode frequency.
- Specialist evaluation is essential if injuries occur or coexisting disorders are suspected.
Ready to rule out airway problems that can spark sleepwalking? Start our free 60‑second AI scan and get clear next steps toward quieter, safer nights.