Two Disorders, One Sleepless Night
Obstructive sleep apnea (OSA) blocks the throat; central sleep apnea (CSA) happens when the brain skips its “breathe” command. Complex sleep apnea (CompSA) is the uneasy mix of both central events emerge or persist while OSA is treated, most often during continuous positive airway pressure (CPAP) titration. Up to 15 % of new CPAP users develop CompSA, according to an American Academy of Sleep Medicine consensus update.
How Treatment‑Emergent CSA Unfolds
The first night on CPAP usually clears throat blockages. Yet in some patients, steady pressure reduces carbon‑dioxide (CO₂) levels so quickly that the brainstem’s breathing pacemaker eases off too much. When CO₂ dips below the “apneic threshold,” the diaphragm rests and a central apnea appears. If more than half of all events recorded on CPAP are central, and they last beyond the first follow‑up, clinicians label the pattern CompSA.
Key sequence:
- CPAP opens airway → CO₂ falls
- Brain senses low CO₂ → breath drive slows
- Central apneas surface → oxygen drops → arousal
- Cycle restarts
A detailed mechanism review is available in this PubMed primer on CompSA for those who want the physiology.
Risk Factors That Tip the Balance
| Risk Factor | Why It Matters |
| Heart failure | Cardiac output delays CO₂ feedback, causing over‑corrections. |
| Male sex & age > 60 | Chemoreceptor sensitivity shifts with aging. |
| Chronic opioid therapy | μ‑receptor activity dulls medullary response to CO₂. |
| High CPAP pressures | Greater washout of CO₂ widens swings in ventilation. |
| Altitude residences | Lower barometric pressure narrows CO₂ safety margin. |
A multi‑center prevalence study reports that CompSA persists in roughly 1.5 % of patients after eight weeks, even with well‑fitted masks and normal weight highlighted in the Complex Sleep Apnea Resolution Study.
Telltale Symptoms
- Continued snoring despite CPAP
- Breathing pauses without chest effort (a bed partner may notice)
- Morning headaches and brain fog
- Persistent insomnia or fragmented sleep reports on CPAP download
- CPAP pressure feels “too high,” yet events persist
If these crop up two to four weeks into therapy, it’s time to re‑evaluate.
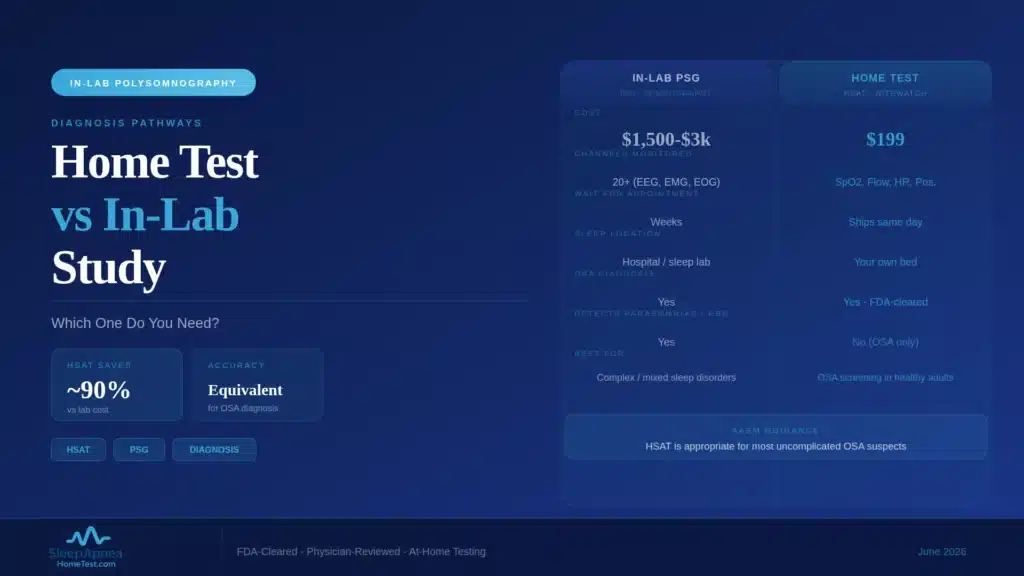
Diagnosis: Beyond Standard Polysomnography
- In‑lab PAP titration confirms that central apneas show up after obstructive events resolve.
- Capnography tracks CO₂ swings; a deep dip before each central pause is typical.
- Multi‑night home testing captures variability that single‑night labs can miss.
- AI facial screening on our site flags craniofacial patterns that predispose to airway collapse start the 60‑second scan to see if you warrant expedited testing.
Therapies Proven to Settle CompSA
Adaptive Servo‑Ventilation (ASV)
Rather than one fixed pressure, ASV watches every breath and adds just enough support to smooth waxing‑waning ventilation. In an ASV efficacy trial, central and mixed apneas fell by over 80 % within one week among PAP‑refractory patients. Note: ASV is not advised for people with severe systolic heart failure; always check with a specialist.
Bilevel PAP with Backup Rate
For users who cannot access ASV, bilevel devices offer a higher inhalation pressure and a timed breath‑trigger if the brain forgets. While not as precise as ASV, bilevel often quells moderate CompSA.
Optimize CPAP Settings
Sometimes, simply reducing fixed pressure or switching to auto‑CPAP stabilizes CO₂ and abolishes central events. A follow‑up study in CHEST showed that 40 % of mild CompSA cases resolve after pressure tweaks alone.
Address Underlying Triggers
- Titrate opioids to the lowest effective dose.
- Manage heart failure aggressively; improved cardiac output shortens feedback delay.
- Consider altitude acclimatization or supplemental oxygen for high‑altitude residents.
Lifestyle Moves That Complement PAP
- Side‑sleeping reduces residual obstructive events and pressure needs.
- Daily aerobic exercise boosts chemoreflex stability within weeks.
- Avoid evening alcohol; it further depresses respiratory drive.
- Consistent bedtimes sync brainstem rhythms with sleep stages, reducing variability in breathing control.
Long‑Term Outlook
Most CompSA resolves within three months when PAP is optimized, but persistence can drive:
- Daytime sleepiness despite adequate hours
- Poor CPAP adherence due to discomfort from cyclic pressures
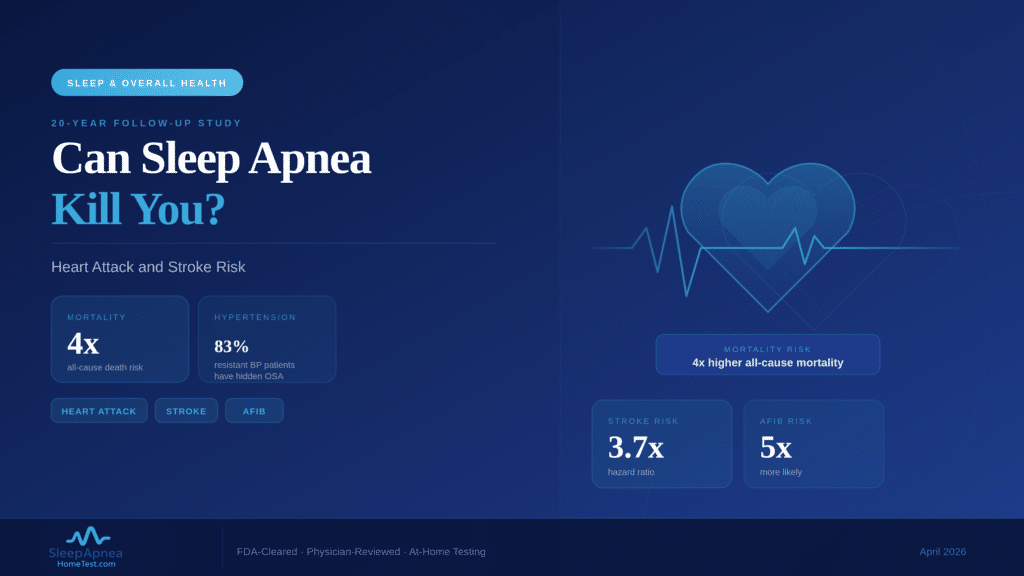
- Higher cardiovascular strain from recurrent desaturations
Regular data downloads and mask‑fit checks every three months keep therapy on track. Emerging tech like phrenic nerve stimulation is under study for stubborn cases, with pilot trials showing promise in lowering residual central apneas (see details in this ASV versus CPAP comparison).
Key Takeaways
- Complex sleep apnea appears when central events emerge while treating OSA with CPAP.
- Heart failure, opioids, high CPAP pressures, and altitude make central pauses more likely.
- ASV is the most effective proven therapy; bilevel with backup rate helps when ASV is off‑limits.
- Fine‑tuning pap settings, managing medical triggers, and adhering to smart sleep habits resolve many cases.
- Early re‑testing plus AI‑based risk screening prevents months of restless nights and maximizes treatment success.
Curious whether your CPAP troubles are really Complex Sleep Apnea? Start our free 60‑second AI scan to see your risk and map out next steps for a steadier night’s sleep.