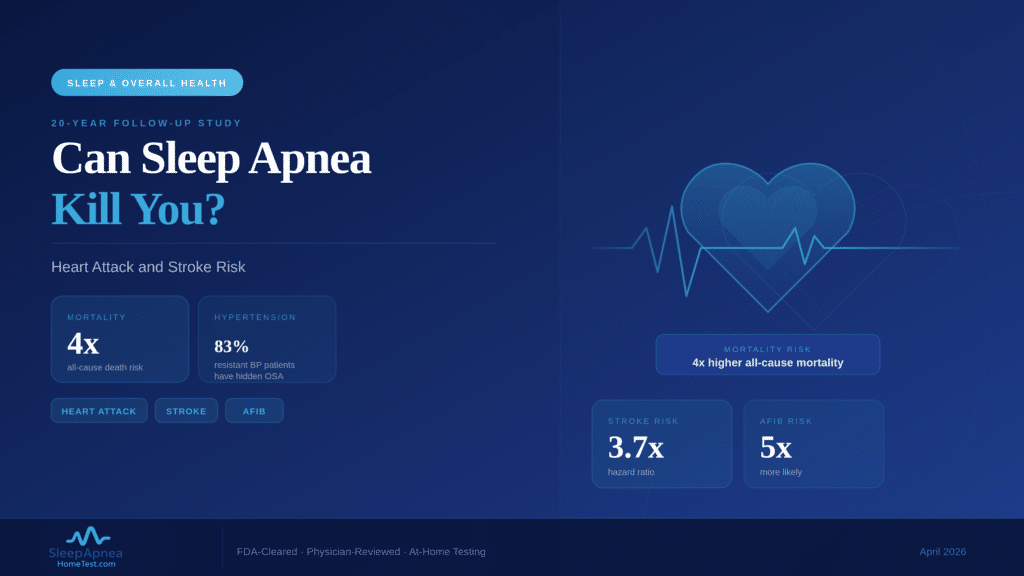
Untreated obstructive sleep apnea increases the risk of dying from any cause by four times, raises the likelihood of stroke by nearly four times, and triples the risk of cancer death, according to a 20-year follow-up study published by the American Academy of Sleep Medicine. People with moderate-to-severe OSA are also five times more likely to develop atrial fibrillation, the most common heart rhythm disorder and a leading cause of stroke. The American Heart Association’s 2026 statistics report lists sleep as a core health behavior alongside smoking, physical activity, and nutrition for cardiovascular health. Sleep apnea is not just a breathing problem. It is a cardiovascular disease in disguise, and testing is the only way to know if you have it.
How Sleep Apnea Damages Your Heart: The Nightly Cycle
Every apnea event triggers a cascade of cardiovascular stress. When breathing stops, blood oxygen drops. The brain detects the oxygen shortage and fires a burst of adrenaline (epinephrine) to restart breathing. This surge spikes blood pressure, accelerates heart rate, and constricts blood vessels. In moderate OSA (AHI 15-29), this cycle repeats 15-29 times per hour. In severe OSA (AHI 30+), it happens 30 or more times per hour, every night, for years.
The cumulative effect is damage to the cardiovascular system at every level. The lining of blood vessels (endothelium) becomes inflamed. Arterial walls stiffen. Platelets become stickier, increasing clot risk. The left ventricle of the heart thickens from repeatedly pumping against constricted vessels. These changes do not reverse themselves. They accumulate, and over years they set the stage for hypertension, coronary artery disease, atrial fibrillation, heart failure, stroke, and sudden cardiac death.
Sleep Apnea Cardiovascular Risk Quick Facts
- All-cause mortality: 4x higher in moderate-to-severe OSA over 20 years (AASM, University of Sydney)
- Stroke risk: Nearly 4x higher (HR 3.7) in moderate-to-severe OSA
- Atrial fibrillation risk: 5x higher in OSA patients (European Society of Cardiology, 2023)
- Sudden cardiac death: OSA shifts peak risk to midnight-6 AM (opposite of the general population)
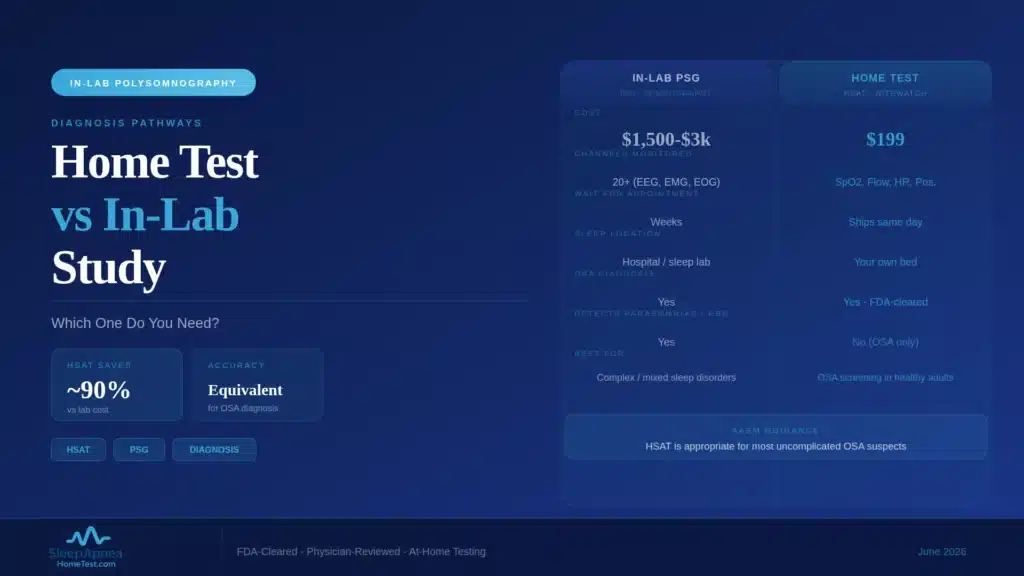
- Resistant hypertension: 83% of patients with drug-resistant high blood pressure have undiagnosed OSA
- Heart failure: OSA causes left ventricular diastolic dysfunction (American Heart Association)
- Cancer death: 3.4x higher in moderate-to-severe OSA (20-year follow-up study)
Hypertension: The Most Common Cardiovascular Consequence
Approximately 50% of people with OSA have hypertension, and approximately 30% of people with hypertension have undiagnosed OSA. The relationship runs both directions, creating a cycle that worsens both conditions. Each apnea-triggered adrenaline surge raises blood pressure acutely, but chronic intermittent hypoxia also resets the sympathetic nervous system to a higher baseline, causing blood pressure to remain elevated during the day even when the patient is breathing normally.
The connection becomes especially critical in treatment-resistant hypertension. Among patients whose blood pressure does not respond to three or more medications, 83% have undiagnosed obstructive sleep apnea. For these patients, adding a fourth drug is less effective than diagnosing and treating the underlying apnea. A home sleep apnea test can identify the hidden driver that blood pressure medications alone cannot address.
The nighttime blood pressure surges during apnea events are especially dangerous. In healthy individuals, blood pressure drops 10-20% during sleep (called “dipping”). People with untreated OSA often lose this dip entirely. This “non-dipping” pattern independently predicts heart attack, stroke, and kidney damage.
Atrial Fibrillation: The Rhythm Disorder That Leads to Stroke
Atrial fibrillation (AFib) is a chaotic heart rhythm where the upper chambers of the heart quiver instead of contracting properly. Blood pools in these chambers, forming clots that can travel to the brain and cause stroke. People with OSA are five times more likely to develop AFib than those without the condition, according to data presented at the European Society of Cardiology conference. The mechanism involves the same oxygen-adrenaline cycle: repeated oxygen drops stretch and remodel the heart’s atrial walls, creating the structural changes that sustain irregular electrical activity.
Even more concerning, OSA patients who undergo treatment for AFib (such as catheter ablation or cardioversion) have much higher recurrence rates if their apnea remains untreated. Cardiology guidelines now recommend screening for OSA in every patient diagnosed with atrial fibrillation. Treating the apnea with CPAP or other therapies reduces AFib recurrence and improves the success rate of cardiac interventions.
Stroke: A Nearly 4x Risk Increase
A 20-year study tracking patients with moderate-to-severe OSA found a hazard ratio of 3.7 for stroke, meaning these patients were nearly four times more likely to suffer a stroke than people without the disorder. The risk operates through multiple pathways: direct vascular damage from repeated oxygen desaturation, increased blood clotting tendency from platelet activation, and the atrial fibrillation pathway described above.
The relationship between sleep apnea and stroke also runs in reverse. Between 6% and 24% of stroke survivors develop central sleep apnea after the event, and OSA worsens stroke outcomes. Patients who have a stroke and also have untreated OSA experience slower neurological recovery, longer hospital stays, and higher rates of recurrent stroke. Identifying and treating sleep apnea before a stroke event is a form of prevention that carries substantial long-term benefit.
Sudden Cardiac Death: Why OSA Reverses the Clock
In the general population, sudden cardiac death peaks between 6 AM and noon, corresponding with the morning surge in blood pressure and cortisol. In people with untreated OSA, the pattern is reversed: it peaks between midnight and 6 AM, when apnea events are most frequent and severe. A study published in the New England Journal of Medicine analyzed over 10,000 adults who underwent sleep studies and found that OSA severity directly correlated with the risk of sudden death during sleep.
The mechanism is the same oxygen deprivation cycle. Severe oxygen drops can trigger fatal arrhythmias, including ventricular fibrillation, and repeated adrenaline surges sensitize the heart muscle to abnormal electrical activity. For patients with existing heart disease, a single severe apnea episode can convert a stable condition into a fatal event. A bed partner who notices prolonged breathing pauses followed by gasping is witnessing events that carry acute cardiac risk. Those events are creating the conditions under which fatal arrhythmias are most likely to occur. Documenting them and getting a home sleep apnea test is a time-sensitive step.
The Diabetes Connection: A Cardiovascular Multiplier
OSA and type 2 diabetes share a bidirectional relationship that amplifies cardiovascular risk. Each apnea event releases stress hormones that reduce insulin sensitivity. Over time, the chronic sleep fragmentation and intermittent hypoxia of untreated OSA increase fasting glucose, raise HbA1c, and promote insulin resistance, even in patients who are not overweight. Research shows that treating OSA with CPAP can lower A1C levels and improve glucose control.
When OSA and diabetes coexist, the cardiovascular risk is not merely additive. The combination creates a reinforcing loop: poor sleep worsens blood sugar, high blood sugar damages blood vessels, damaged blood vessels increase blood pressure, and elevated blood pressure compounds the cardiac stress caused by apnea events. Treating the apnea interrupts this cycle at its source.
What CPAP Treatment Does for Heart Risk
CPAP therapy eliminates apnea events by holding the airway open with continuous air pressure. When used consistently (at least 4 hours per night, though more is better), CPAP has been shown to reduce blood pressure by 2-7 mmHg, restore the normal nighttime blood pressure dip, reduce AFib recurrence after cardioversion or ablation, improve ejection fraction in heart failure patients, and shift sudden cardiac death risk away from the midnight-6 AM window. The cardiovascular benefits of CPAP are dose-dependent: patients who use it for 6+ hours per night see greater improvements than those who use it for 4 hours.
For patients who cannot tolerate CPAP, alternatives include APAP machines with auto-adjusting pressure, oral appliances for mild-to-moderate cases, positional therapy for supine-dominant apnea, and weight management. The critical factor is reducing the AHI to lower the nightly cardiovascular burden.
Who Is at Highest Risk?
Certain groups face compounded cardiovascular danger from undiagnosed sleep apnea.
Adults over 50 with high blood pressure: If your blood pressure requires two or more medications and still is not controlled, undiagnosed sleep apnea is a likely contributor. Testing should be a standard part of your workup.
People with existing heart disease: OSA worsens outcomes for coronary artery disease, heart failure, and post-surgical cardiac recovery. Identifying it before a cardiac event improves both treatment planning and long-term survival.
Men with a neck circumference over 17 inches and women over 16 inches: Neck size is one of the strongest physical predictors of OSA. Combined with symptoms like snoring, daytime fatigue, or morning headaches, it warrants testing.
People with a family history of stroke or heart attack before age 65: If cardiovascular disease runs in your family, addressing modifiable risk factors becomes even more critical. Untreated sleep apnea is one of the most modifiable risks available.
Women, who are significantly underdiagnosed: OSA in women often presents with fatigue, insomnia, and mood changes rather than loud snoring. This atypical presentation leads to missed diagnoses and untreated cardiovascular risk.
What This Means for You
The data is direct: untreated sleep apnea damages your heart and blood vessels every single night, and the damage accumulates over years. The 20-year mortality data (4x all-cause death risk), the stroke numbers (nearly 4x), and the AFib connection (5x) are not abstract population statistics. They represent the trajectory of an untreated condition that affects roughly 30 million Americans, 80% of whom remain undiagnosed.
The encouraging counterpoint is that treatment works. CPAP use reduces blood pressure, lowers AFib recurrence, and shifts sudden cardiac death risk away from the dangerous overnight window. Even partial treatment yields measurable benefit: patients who use CPAP for 4+ hours per night show significant cardiovascular improvements compared to those who do not treat their OSA at all. Patients who use it for 6+ hours see even greater gains.
Testing is the single action that separates “maybe I snore a lot” from “I have a measurable, treatable condition.” A confirmed AHI number puts you on a path to treatment that reduces every cardiovascular risk described above. If your AHI comes back normal, the test has ruled out one of the most dangerous modifiable risk factors for heart disease and stroke, and that information has value too.
Frequently Asked Questions
Can sleep apnea actually kill you?
Yes. A 20-year follow-up study published by the American Academy of Sleep Medicine found moderate-to-severe OSA carries a 4x higher all-cause mortality rate and a hazard ratio of 3.7 for stroke. Sudden cardiac death risk also shifts into the overnight hours for OSA patients. The damage is cumulative, and every untreated year adds cardiovascular risk.
Does CPAP reduce heart attack and stroke risk?
CPAP reduces blood pressure by 2-7 mmHg when used consistently, restores the normal nighttime blood pressure dip, reduces atrial fibrillation recurrence after cardiac procedures, and shifts sudden cardiac death risk out of the high-risk midnight-6 AM window. Benefits are dose-dependent: 6+ hours per night gives greater protection than the 4-hour insurance-compliance minimum.
What is the connection between sleep apnea and atrial fibrillation?
People with OSA are roughly 5 times more likely to develop atrial fibrillation, per European Society of Cardiology data. Repeated oxygen drops stretch and remodel the atrial walls, creating the structural changes that sustain irregular rhythm. AFib patients with untreated OSA have much higher recurrence rates after ablation or cardioversion, so cardiology guidelines now recommend OSA screening in every AFib diagnosis.
Why does sudden cardiac death happen more often during sleep with OSA?
In the general population, sudden cardiac death peaks 6 AM-noon with the morning adrenaline surge. In OSA patients, it peaks midnight-6 AM, the hours when apnea events are most frequent and severe. Severe oxygen drops can trigger fatal arrhythmias including ventricular fibrillation, and repeated adrenaline surges sensitize the heart muscle to abnormal electrical activity. If a bed partner has witnessed gasping or choking episodes, a home sleep apnea test measures how often and how severe these events are.
My blood pressure medications are not working. Could it be sleep apnea?
Likely. Among patients whose blood pressure does not respond to three or more medications, 83% have undiagnosed OSA. Adding a fourth drug is typically less effective than diagnosing and treating the underlying apnea. An FDA-cleared home sleep test can identify the hidden driver that blood pressure medications alone cannot address.
Next Steps
Your cardiovascular health deserves a clear answer. Take the free 30-second AI facial scan to assess your OSA risk. If your risk is elevated, order the FDA-cleared home sleep test kit to get your AHI score. Your test includes: an FDA-cleared overnight monitoring device that tracks AHI, SpO2, and airflow, a diagnostic report reviewed and signed by a board-certified sleep physician, and guidance on treatment options matched to your severity.
Medical disclaimer: This article is for educational purposes and does not constitute medical advice. If you are experiencing chest pain, shortness of breath, or other symptoms of a cardiac emergency, call 911 immediately. Consult a licensed healthcare provider for guidance on sleep apnea diagnosis and treatment.