A study published in JAMA Neurology in November 2025, analyzing health records from more than 11 million U.S. military veterans over 23 years, found that people with untreated obstructive sleep apnea were nearly twice as likely to develop Parkinson’s disease as those who used CPAP therapy. The finding held even after researchers controlled for obesity, age, and high blood pressure. This is the largest study ever to examine the relationship between OSA and Parkinson’s, and it adds neurodegenerative disease to the list of serious health consequences linked to leaving sleep apnea untreated.
The Study: Scale, Methods, and Key Numbers
Researchers from Oregon Health & Science University (OHSU) and the Portland VA Health Care System led the project. They examined electronic health records from 11 million+ veterans who received care through the Department of Veterans Affairs between 1999 and 2022. The study identified veterans with a documented OSA diagnosis and tracked whether they had been prescribed and were using CPAP. The primary outcome was a new Parkinson’s disease diagnosis during the follow-up period.
After adjusting for known confounders (age, BMI, hypertension, and other comorbidities), veterans with untreated sleep apnea had nearly double the likelihood of a Parkinson’s diagnosis compared to those using CPAP. Lead author Dr. Lee Neilson, assistant professor of neurology at OHSU, summarized the mechanism: repeated nightly drops in oxygen likely strain neurons over time. When breathing stops and oxygen falls, neurons cannot function at normal levels. Accumulated over years and decades, this stress may contribute to the kind of cell death seen in Parkinson’s.
Sleep Apnea and Parkinson’s Quick Facts
- Study size: 11 million+ U.S. military veterans (1999-2022)
- Publication: JAMA Neurology, November 24, 2025
- Lead institution: Oregon Health & Science University (OHSU)
- Key finding: Untreated OSA nearly doubled the odds of Parkinson’s diagnosis
- Protective factor: CPAP use cut Parkinson’s risk by nearly half
- Controls: Age, obesity, high blood pressure, other comorbidities
- Parkinson’s prevalence: Approximately 1 million Americans, rising after age 60
How Oxygen Deprivation May Damage the Brain Over Time
The brain consumes roughly 20% of the body’s oxygen supply despite making up only 2% of body weight. Neurons in the substantia nigra, the brain region that produces dopamine and degenerates in Parkinson’s disease, are especially sensitive to oxygen fluctuations. Every apnea event, a pause in breathing lasting 10 seconds or longer, triggers a temporary drop in blood oxygen. In moderate OSA (AHI 15-29), this happens 15-29 times per hour. In severe OSA (AHI 30+), it happens 30 or more times per hour, every single night.
Researchers describe the damage as cumulative oxidative stress. Each oxygen drop generates reactive oxygen species (free radicals) that damage cell membranes and DNA. The body’s repair mechanisms can handle occasional insults, but hundreds of events per night, year after year, may overwhelm these defenses. Dr. Gregory Scott, co-author and assistant professor of pathology at OHSU, noted that the link represents a measurable increase in odds that accumulates over time. This oxygen-deprivation pathway also connects to other conditions linked to untreated OSA, including blood pressure surges and glucose control problems.
Why CPAP Appears Protective Against Parkinson’s
CPAP maintains continuous airflow throughout the night, preventing the airway collapses that cause oxygen desaturation events. By keeping oxygen levels stable, CPAP eliminates the primary mechanism researchers believe connects OSA to neurodegeneration. The JAMA Neurology study found that veterans who consistently used their CPAP had Parkinson’s rates markedly lower than those who were diagnosed with OSA but did not treat it.
Dr. Scott noted that veterans who use their CPAP tend to become strong advocates for the therapy. They report feeling more rested, more alert, and less fatigued. If the Parkinson’s risk reduction becomes widely understood, it could motivate more patients to commit to nightly CPAP use, a persistent challenge in sleep medicine. Current CPAP adherence rates hover around 50%, meaning roughly half of people prescribed CPAP do not use it consistently.
For those who find CPAP difficult to tolerate, alternatives exist: APAP machines that auto-adjust pressure, oral appliances for mild-to-moderate cases, and positional therapy for supine-dominant apnea. The critical factor is treating the apnea to maintain oxygen levels, regardless of the specific device used.
Early Treatment Yields Greater Benefit
The study’s timeline (1999-2022) allows researchers to observe the effects of long-term CPAP use versus long-term non-treatment. Veterans who started CPAP earlier in their OSA journey showed a larger gap in Parkinson’s risk reduction compared to those who began treatment later. This aligns with the cumulative-damage hypothesis: if each untreated year adds incremental neuronal stress, then every year of treatment prevents that year’s damage from accruing.
For patients in their 40s and 50s diagnosed with OSA, this carries practical urgency. Waiting five years to start treatment is not merely five years of poor sleep. It is five years of nightly oxygen deprivation acting on vulnerable brain regions. Starting treatment at 45 instead of 50 could mean entering the high-risk Parkinson’s window (age 60+) with a healthier neurological baseline. The home sleep test that costs $199 today may prevent neurological decline that compounds for decades.
The Broader Picture: OSA as a Systemic Disease
This study reinforces that obstructive sleep apnea is not just a sleep problem. Untreated OSA is already linked to:
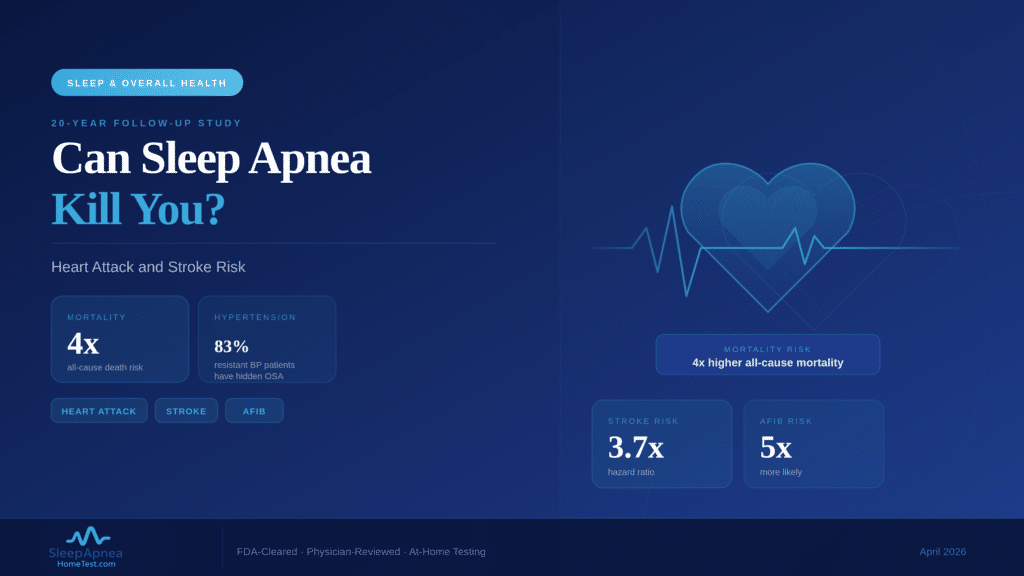
Cardiovascular disease: Repeated blood pressure surges during apnea events stress the heart and blood vessels, increasing the risk of hypertension, atrial fibrillation, heart failure, and stroke.
Metabolic dysfunction: OSA disrupts glucose regulation and alters appetite hormones, contributing to type 2 diabetes and weight gain in a vicious cycle.
Mental health: Untreated apnea mimics depression symptoms and impairs cognitive function. CPAP compliance has been shown to improve mood across multiple studies.
Neurodegeneration: The 2025 JAMA Neurology study now adds Parkinson’s disease to this list, with a separate 2025 study linking REM-stage OSA to memory-related brain changes.
The common thread across all these conditions is intermittent hypoxia: the repeated oxygen drops that occur with each untreated apnea event. Treating the apnea addresses the root cause rather than chasing individual symptoms.
Sleep Apnea and REM-Stage Brain Damage
A separate 2025 study found that obstructive sleep apnea occurring during REM sleep is specifically linked to degeneration of brain regions involved in memory. During REM, the brain is highly active and vulnerable to oxygen fluctuations. Apnea events during this stage damage the brain’s small blood vessels, particularly in the hippocampus and surrounding structures that consolidate new memories.
REM-stage apnea is especially concerning because REM periods grow longer in the second half of the night. Patients who use CPAP for only the first 4 hours (the insurance-compliance minimum) may still be unprotected during the longest REM cycles. This supports the consensus that 6-8 hours of CPAP use per night provides meaningfully greater brain protection than 4 hours. The combination of the Parkinson’s finding and the REM-memory study points to the same conclusion: the brain pays a cumulative price for every untreated apnea event. A home sleep apnea test measures how often those events occur and how urgently treatment should begin.
What the Veterans Study Cannot Tell Us
The JAMA Neurology study is observational, not experimental. Researchers analyzed existing medical records and compared outcomes between groups rather than randomly assigning patients to treatment. This design identifies strong associations but cannot prove that untreated OSA directly causes Parkinson’s. Factors not captured in electronic health records, such as environmental toxin exposure, dietary patterns, or genetic predisposition, may also contribute.
That said, the study’s scale (11 million+ veterans over 23 years) and consistency after controlling for age, obesity, and hypertension give the findings substantial weight. The biological plausibility is strong: the substantia nigra is known to be sensitive to oxidative stress, and repeated oxygen deprivation generates exactly that. Researchers at OHSU have called for prospective studies with detailed brain imaging to strengthen the causal case.
For patients deciding whether to get tested today, the question is practical. Treating sleep apnea improves daytime alertness, reduces cardiovascular risk, improves mood, and now appears to reduce neurodegenerative risk. The cost of testing is $199. The cost of not testing accumulates every night.
Who Should Pay Closest Attention
Parkinson’s risk rises after age 60, while sleep apnea prevalence increases with age and is most common in adults over 35. The overlap window, people in their 40s, 50s, and 60s with undiagnosed sleep apnea, represents the group most likely to benefit from early testing and treatment. Other risk factors for OSA include a neck circumference above 17 inches, a family history of sleep apnea, male sex (though women are significantly underdiagnosed), and excess body weight.
If you snore, wake up gasping, experience morning headaches, or feel excessively tired despite sleeping 7-8 hours, these are signals worth investigating. The cumulative damage described in the Parkinson’s study is measured in decades, which means the sooner treatment begins, the more years of neuroprotection you gain.
What This Means for You
The JAMA Neurology study does not mean every person with sleep apnea will develop Parkinson’s. It means that untreated OSA carries a measurable and preventable increase in risk. CPAP and other treatments appear to substantially reduce that risk. The first step is finding out whether you have sleep apnea at all. A $199 home sleep test today could change the trajectory of your neurological health over the next 20 years.
Frequently Asked Questions
Does untreated sleep apnea cause Parkinson’s disease?
The JAMA Neurology study of 11 million+ veterans found untreated OSA was associated with nearly double the risk of Parkinson’s diagnosis after controlling for age, obesity, and hypertension. The study is observational, so it shows strong association rather than proven causation. The proposed mechanism is cumulative oxidative stress from repeated nighttime oxygen drops damaging dopamine-producing neurons in the substantia nigra.
Can using CPAP reduce my Parkinson’s risk?
Veterans in the JAMA Neurology study who used CPAP consistently had markedly lower Parkinson’s rates than those who were diagnosed with OSA but did not treat it. Earlier and longer CPAP use showed the greatest benefit. Adherence matters: consistent nightly use of 6-8 hours gives more protection than the 4-hour insurance-compliance minimum. Confirming your apnea severity with a home sleep test is the starting point for measuring how much protection CPAP gives you.
At what age should I worry about sleep apnea and Parkinson’s?
Parkinson’s risk rises sharply after age 60, while OSA prevalence climbs from age 35 onward. The overlap window, people in their 40s, 50s, and 60s with undiagnosed OSA, represents the group with the most to gain from early testing. Starting treatment at 45 instead of 50 can protect five additional years of vulnerable neurons.
What symptoms suggest I should get tested?
Loud snoring, witnessed breathing pauses, gasping or choking during sleep, morning headaches, excessive daytime tiredness despite adequate time in bed, and a neck circumference above 17 inches (men) or 16 inches (women) are the strongest indicators. Women often present atypically with fatigue and insomnia rather than snoring and are underdiagnosed as a result.
How do I find out if I have sleep apnea?
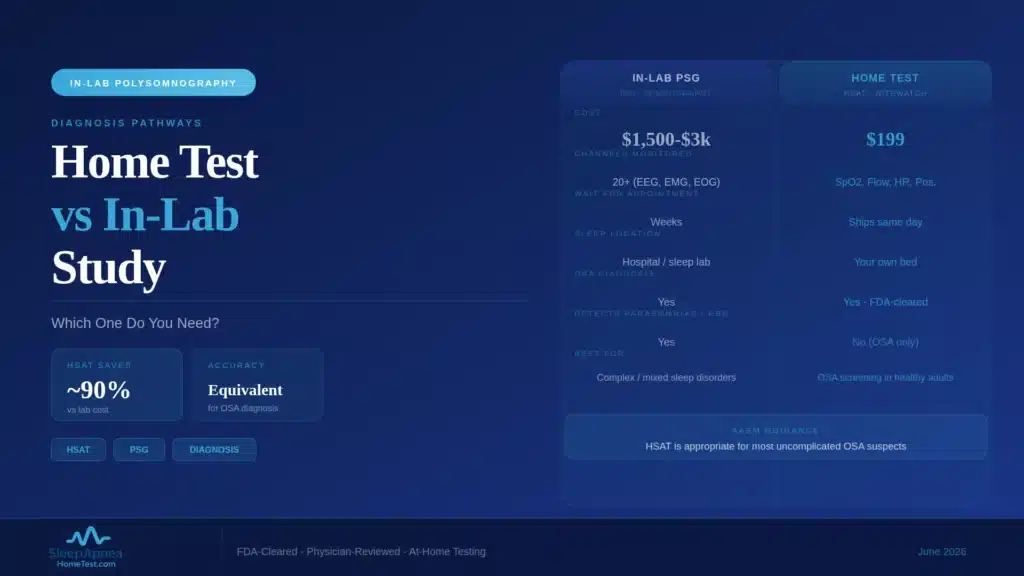
Start with a free 30-second AI facial scan to gauge your risk level. If elevated, an FDA-cleared home sleep test measures your AHI, oxygen saturation, and airflow overnight in your own bed. A board-certified sleep physician reviews the data and delivers a diagnostic report, typically within days.
Next Steps
Knowing your sleep apnea status is the first step toward protecting your brain, heart, and overall health. Take the free 30-second AI facial scan to assess your risk. If your risk is elevated, the home sleep test kit gives you a physician-reviewed AHI score and diagnostic report. Your test includes: an FDA-cleared overnight monitoring device, measurement of AHI, SpO2, and airflow, and a diagnostic report signed by a board-certified sleep physician.
Medical disclaimer: This article is for educational purposes and does not constitute medical advice. Consult a licensed healthcare provider for guidance on sleep apnea diagnosis and treatment.