By Dr. Joshua Roland, MD, FAASM
When a home sleep test is the right diagnostic, when in-lab polysomnography is needed, and how to know which applies to you.
For uncomplicated adults at increased risk of moderate-to-severe obstructive sleep apnea, the American Academy of Sleep Medicine endorses a home sleep apnea test as a valid first-line alternative to an in-lab sleep study, at roughly one-tenth the out-of-pocket cost. It is not the right test for everyone. The decision comes down to one question a physician asks before ordering anything: how complex is this patient’s clinical picture? This article walks through how that decision is made, so you can recognize which path fits your situation.
Quick Facts
- HSAT vs PSG: AASM-endorsed first-line alternative for uncomplicated moderate-to-severe OSA; a negative or inconclusive home test should be followed by PSG
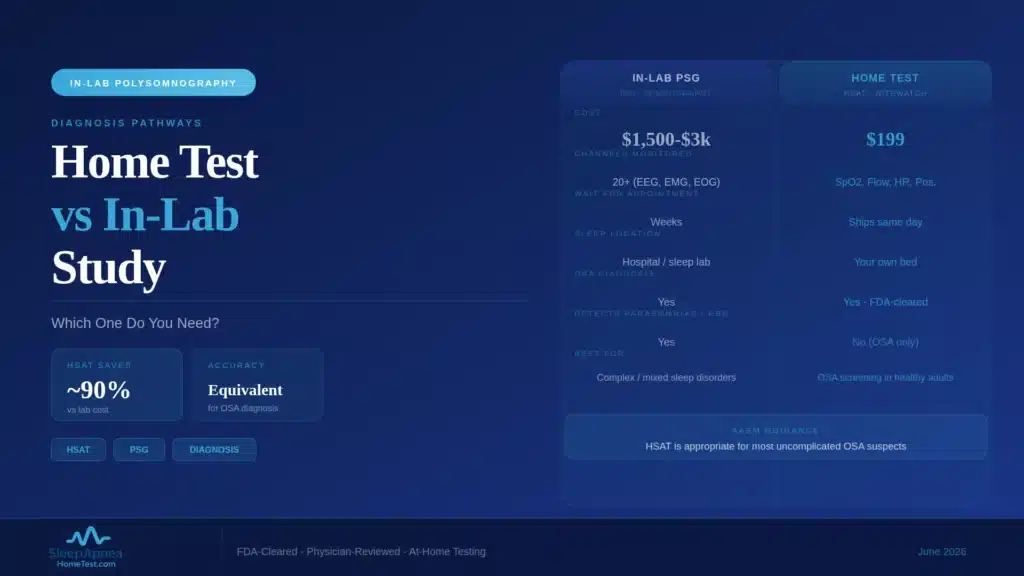
- Out-of-pocket cost: home sleep apnea test $199; in-lab polysomnography $1,500 to $3,000
- AASM position: HSAT is first-line for uncomplicated suspected OSA in adults
- Sleep stages measured: HSAT typically none or limited; PSG measures all stages
- Recording channels: HSAT 6; PSG 12 or more
- Turnaround: HSAT results in 2 to 7 days; PSG results in 2 to 4 weeks
What a Home Sleep Apnea Test Measures, and What It Does Not
A Type III home sleep apnea test records the physiological signals that matter most for obstructive sleep apnea: airflow, respiratory effort, oxygen saturation, and pulse. The NiteWatch device records six channels, which is at the upper end of the home-test range. From those signals, the test calculates your Apnea-Hypopnea Index, the count of breathing interruptions per hour that defines OSA severity.
What a home test does not do is measure sleep itself. It cannot tell, with the precision of a lab study, when you were asleep versus lying awake, or how your night divided across REM and the non-REM stages. Because it estimates time in bed rather than confirmed sleep time, a home test can slightly underestimate severity in someone who slept poorly during the recording. For straightforward OSA, that limitation rarely changes the treatment decision. For more complex sleep complaints, it can.
When In-Lab Polysomnography Is the Right Call
In-lab polysomnography remains the correct test for several specific situations, and a careful physician will route you there rather than to a home test. An attended lab study is indicated when you have significant cardiopulmonary disease such as moderate-to-severe heart failure or COPD, a history of stroke, or neuromuscular disease, because these conditions both raise the stakes and degrade home-test accuracy.
A lab study is also the right call when central sleep apnea is suspected rather than obstructive, when the clinical picture points to a non-respiratory sleep disorder such as narcolepsy or a parasomnia, or when a prior home test was negative but symptoms persist. Lab studies are also used for CPAP titration, the process of finding the exact pressure that resolves your events. The lab is not a better test in some abstract sense. It is the right tool when the question is more complicated than “does this person have obstructive sleep apnea.”
The AASM Guideline Position
The American Academy of Sleep Medicine has been clear on this for over a decade. Its clinical practice guideline supports home sleep apnea testing as a first-line diagnostic for adults with a high pretest probability of moderate-to-severe obstructive sleep apnea and no significant comorbidity. The same guideline directs patients with the comorbidities described above to in-lab testing.
The reasoning is practical. Most patients evaluated for sleep apnea have uncomplicated OSA, the home test answers the question accurately for that majority, and reserving lab capacity for complex cases shortens the wait for everyone. The guideline is not a cost-cutting compromise. It reflects where each test performs best.
The Cost and Insurance Reality
The price gap between the two tests is large and worth understanding before you choose a path. A home sleep apnea test runs $199 out of pocket. An in-lab polysomnogram runs $1,500 to $3,000 before insurance, and even with coverage the copay and deductible exposure is usually higher than the full cash price of a home test.
Most commercial insurance plans, Medicare, and Medicaid cover home sleep apnea testing when a physician orders it for suspected OSA, often with the home test required first before a lab study is authorized. If you are weighing the two, verifying your benefits early prevents an expensive surprise. You can submit your insurance information for a free coverage check before paying anything out of pocket.
The Patient Experience, Compared
The two tests feel very different. An in-lab study means a night away from home, in an unfamiliar bed, wired to roughly two dozen sensors, with a technologist monitoring from another room. Many people sleep worse than usual under those conditions, which is the well-known “first-night effect.” The tradeoff is a complete, attended recording with a technologist who can fix a loose sensor in real time.
A home test means sleeping in your own bed, on your own schedule, with a small device you apply yourself in under ten minutes. Most people sleep more naturally, which is part of why home results track real life well. The tradeoff is that if a sensor slips, no one is there to correct it, so a small fraction of home recordings need a second night.
When a Negative Home Test Does Not Rule Out Sleep Apnea
A negative or borderline home sleep apnea test is not always the final word, and this is the point I most want patients to understand. Because a home test can underestimate severity when sleep is fragmented or when REM sleep is scarce during the recording, a person with genuine OSA can occasionally score in the normal range on a single home night.
If your home test is negative but you still have loud snoring, witnessed pauses in breathing, or persistent daytime sleepiness, tell the reviewing physician. The appropriate next step is often an in-lab study, which captures a full night of confirmed sleep and is harder to fool. A negative result with ongoing symptoms is a reason to keep investigating, not to stop. If your circumstances or symptoms point you toward testing, a home sleep test is a reasonable and low-barrier place to start the conversation with a physician.
How I Decide Which Test to Order
When I see a patient with suspected sleep apnea, the decision follows a short internal checklist. First, what is the pretest probability: do the symptoms and risk factors strongly suggest OSA? Second, are there comorbidities, heart failure, severe lung disease, prior stroke, neuromuscular disease, or opioid use, that raise the stakes or degrade home-test accuracy? Third, is there anything in the history that suggests a non-OSA sleep disorder?
If the probability of OSA is high and there are no complicating factors, a home sleep apnea test is the efficient, accurate, patient-friendly choice. If any complicating factor is present, the lab is the right call from the start. The goal is never to default to one test. It is to match the test to the patient.
What a Home Test Result Actually Tells You
Patients sometimes expect a sleep test to deliver a simple yes or no. The real output is more useful than that. A home sleep apnea test produces an Apnea-Hypopnea Index, the number of breathing events per hour, and that number places you in a severity band: an AHI under 5 is normal, 5 to 14 is mild, 15 to 29 is moderate, and 30 or higher is severe. The report also describes how far your oxygen level dropped during events and how often.
That severity grade is what drives the next decision. Mild OSA is sometimes managed with positional therapy or weight management; moderate-to-severe OSA usually warrants CPAP or another active treatment. The AHI also serves as your baseline, the number against which any future treatment is measured. So a home test does not just answer whether you have sleep apnea. It tells the physician how significant it is and gives both of you a figure to track. If your symptoms point that way, ordering a home sleep test is a reasonable way to get that number.
Frequently Asked Questions
Is a home sleep apnea test as accurate as a sleep lab study?
For uncomplicated adults at increased risk of moderate-to-severe obstructive sleep apnea, the AASM endorses a home sleep apnea test as a valid first-line alternative to an in-lab study. The guideline also specifies that a negative, inconclusive, or technically inadequate home test should be followed by polysomnography. For complex cases or suspected non-obstructive sleep disorders, the lab study remains the more appropriate test.
When does my doctor need to order an in-lab study instead?
An in-lab study is indicated for significant heart failure or COPD, prior stroke, neuromuscular disease, suspected central sleep apnea, or when a non-respiratory sleep disorder such as narcolepsy is on the table. It is also used for CPAP pressure titration and when a prior home test was negative but symptoms continue.
Does insurance cover home sleep apnea testing?
Most commercial plans, Medicare, and Medicaid cover home sleep apnea testing when a physician orders it for suspected OSA. Many plans now require the home test first before authorizing a lab study. You can verify your specific benefits before any charge.
How long does the home test recording need to be?
A home sleep apnea test typically records one full night, ideally with at least four hours of sleep. If the first night produces unclear data, a second night is recorded. The reviewing physician needs enough confirmed recording time to calculate a reliable Apnea-Hypopnea Index.
What happens if my home test results are inconclusive?
If the recording does not yield clear results, the next step is usually a second night of home recording or referral for an in-lab study. A reputable provider includes that follow-up at no additional physician-review fee, because an inconclusive first night is a known and manageable outcome, not a dead end.
Can children use home sleep apnea tests?
Home sleep apnea tests are validated primarily in adults. Pediatric sleep apnea is evaluated differently, and most children with suspected OSA are referred for in-lab polysomnography, which captures the full picture children’s sleep requires. A pediatric sleep specialist should guide testing for anyone under 18, rather than an adult home test.
What conditions disqualify someone from home sleep testing?
Moderate-to-severe heart failure, significant COPD or other serious lung disease, prior stroke, neuromuscular disease, chronic opioid use, and suspected central sleep apnea all point away from a home test and toward an attended lab study. The intake questionnaire screens for these so the right test is ordered from the start. If none apply, a home sleep test is a reasonable first step.
Content on SleepApneaHomeTest.com is for educational and screening purposes and does not replace consultation with your own physician. The NiteWatch home sleep apnea test is FDA-cleared for the diagnosis of obstructive sleep apnea in adults; results are reviewed by a board-certified sleep medicine physician licensed in the patient’s state of residence.