By Dr. Joshua Roland, MD, FAASM
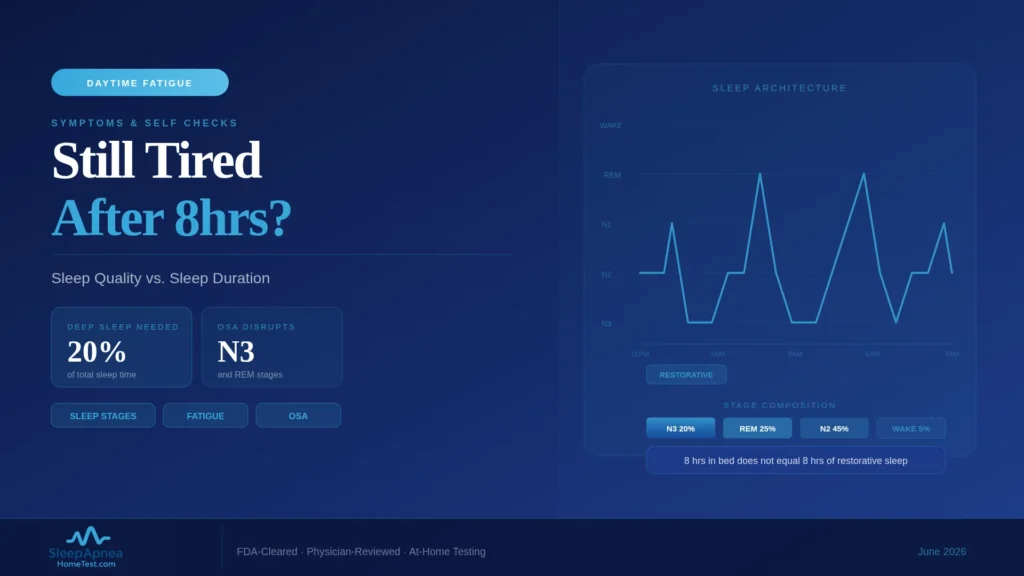
Eight hours in bed does not mean eight hours of restorative sleep. Here is what determines sleep quality and why duration alone misleads.
If you spend 8 hours in bed and still wake up exhausted, the problem is usually not how long you slept but how well. Time in bed and restorative sleep are different measurements, and the gap between them is where most unexplained daytime tiredness lives. As a sleep physician, this is one of the most common complaints I hear, and the answer is rarely “sleep more.” It is usually “find out what is fragmenting the sleep you are already getting.”
Quick Facts
- Time in bed and total sleep time are different metrics: you can lie down for 8 hours and sleep far less
- Sleep architecture matters: restorative sleep depends on cycling properly through REM and the N1, N2, and N3 stages
- Common quality disruptors: obstructive sleep apnea, periodic limb movements, and frequent brief arousals
- The Epworth Sleepiness Scale is a standard self-rating tool; higher scores suggest excessive daytime sleepiness
- Persistent daytime sleepiness despite adequate time in bed is a signal of a sleep disorder, not normal tiredness
The Duration-Versus-Quality Distinction
Most advice about sleep focuses on a single number: get seven to nine hours. Duration matters, but it is only half the equation. Two people can each spend eight hours in bed and wake up in completely different states, because what restores you is not time in bed, it is time in genuine, well-structured sleep.
Sleep scientists separate these with specific terms. Time in bed is exactly that, the clock running from lights-out to getting up. Total sleep time is the portion of that you were actually asleep. Sleep efficiency is the ratio between them. Someone with an apparently normal eight hours in bed but a sleep efficiency dragged down by frequent awakenings may be getting six hours of actual, choppy sleep, and feeling every bit of the deficit. The number on the alarm clock does not capture this. That is why “I slept eight hours and I’m still wrecked” is not a contradiction.
Sleep Architecture and Why It Matters
Healthy sleep is not a uniform block. It is a structured progression through stages that repeats 4 to 6 times a night. Light sleep, stages N1 and N2, makes up the largest share at roughly 50 to 60 percent of the night and serves as connective tissue between deeper states. Deep sleep, N3 or slow-wave sleep, makes up about 13 to 23 percent, is concentrated early in the night, and is when the body does much of its physical restoration. REM sleep, around 20 to 25 percent and weighted toward the second half of the night, supports memory and emotional processing.
A restorative night moves through these stages in roughly 90-minute cycles, with the right proportions of each. When something repeatedly interrupts that progression, the architecture fragments. You may technically accumulate 8 hours, but if you keep getting pulled out of deep sleep or REM before completing a cycle, the sleep does not deliver what it should. This is why architecture, not just duration, determines how you feel.
Common Causes of Poor-Quality Sleep at Adequate Duration
When someone reports sleeping enough hours but waking unrefreshed, a sleep physician runs through a short list of usual suspects. Obstructive sleep apnea is at the top, and the next section covers it specifically. Periodic limb movement disorder, in which the legs twitch repeatedly through the night, can fragment sleep without the sleeper being aware. Restless legs syndrome delays sleep onset and disrupts it.
Beyond sleep disorders proper, several common factors degrade quality. Alcohol close to bedtime suppresses REM sleep and causes mid-night awakenings. Some medications alter sleep architecture. Chronic stress and pain produce frequent micro-arousals. An irregular schedule keeps the body’s clock unsettled. Caffeine late in the day extends sleep onset and reduces deep sleep even when you do fall asleep. Any of these can leave a full eight hours feeling hollow.
The Role of Sleep Apnea in Daytime Fatigue
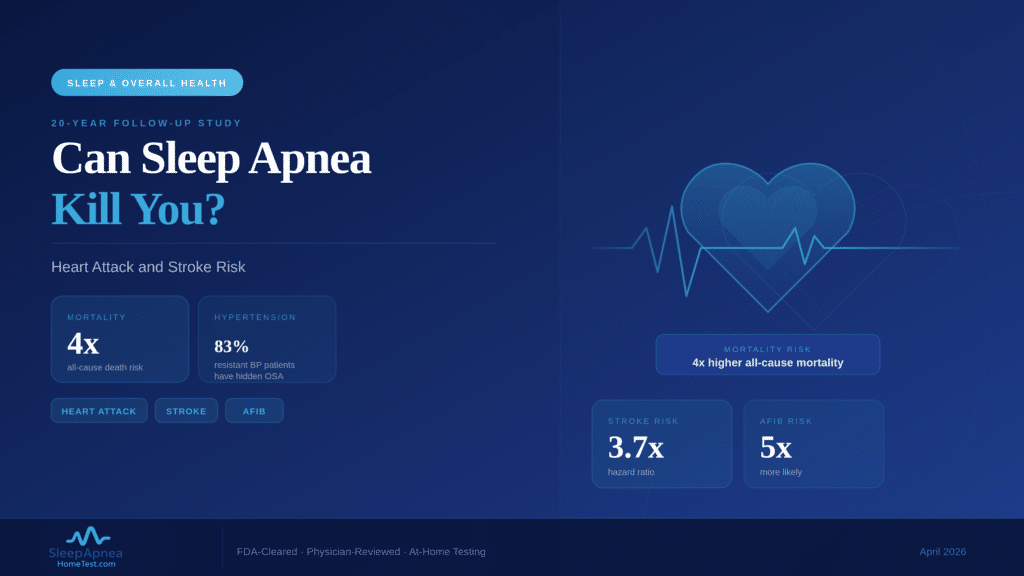
Of all the causes of unrefreshing sleep, obstructive sleep apnea deserves particular attention, because it is common, frequently undiagnosed, and one of the most direct destroyers of sleep quality. In OSA, the airway repeatedly narrows or closes during sleep. Each event ends in a brief arousal, often too short to remember, as the body reopens the airway.
A person with moderate or severe OSA can experience these events dozens of times an hour. The result is sleep that is shredded into fragments and chronically starved of the deep and REM stages, even across a full night in bed. The sleeper has no memory of the interruptions and reasonably concludes they slept fine, which is exactly why OSA is so often missed. The daytime sleepiness is real and the cause is hidden. A home sleep apnea test is a straightforward way to find out whether this is what is happening to your nights.
Hypersomnia and Idiopathic Hypersomnia
Not all excessive sleepiness traces to fragmented sleep. In a smaller group of patients, the sleep itself is intact, plenty of it, structurally sound, and the person is still profoundly sleepy. This points toward a central disorder of hypersomnolence.
Idiopathic hypersomnia is the clearest example. People with it sleep long hours, often more than the typical range, do not have apnea or another fragmenting condition, and yet remain heavily sleepy during the day, frequently with severe “sleep drunkenness” on waking. Narcolepsy is the better-known central hypersomnia. These conditions are diagnosed differently from OSA, often requiring specialized daytime testing such as the Multiple Sleep Latency Test, and they are why a sleep evaluation does not stop at ruling out apnea. If the sleep is genuinely sufficient and undisturbed and the sleepiness persists, the investigation continues.
When to Pursue a Formal Sleep Evaluation
There is a reasonable threshold for moving from self-management to a medical evaluation. If you consistently get seven to nine hours in bed, keep a regular schedule, and still feel sleepy enough that it affects your driving, your work, your mood, or your safety, that is not ordinary tiredness and it warrants evaluation.
Specific red flags lower that threshold further: a bed partner reporting snoring, gasping, or pauses in your breathing; falling asleep unintentionally during the day; morning headaches; or sleepiness severe enough to be dangerous behind the wheel. Persistent, unexplained daytime sleepiness is a symptom, and like any symptom it deserves a diagnosis rather than indefinite tolerance.
Self-Screening Tools
Two simple tools can help you gauge whether your tiredness merits attention. The Epworth Sleepiness Scale asks how likely you are to doze in eight everyday situations, such as reading or sitting in traffic. A higher total score points toward genuine excessive daytime sleepiness rather than ordinary fatigue.
The STOP-BANG questionnaire screens specifically for obstructive sleep apnea risk, asking about snoring, tiredness, observed breathing pauses, blood pressure, body mass index, age, neck size, and sex. A higher STOP-BANG score raises the probability of OSA and is a reason to pursue testing. Neither tool is a diagnosis; both are useful for deciding whether to take the next step. You can check your STOP-BANG-based risk score in a couple of minutes as a starting point.
From Screening to Answers
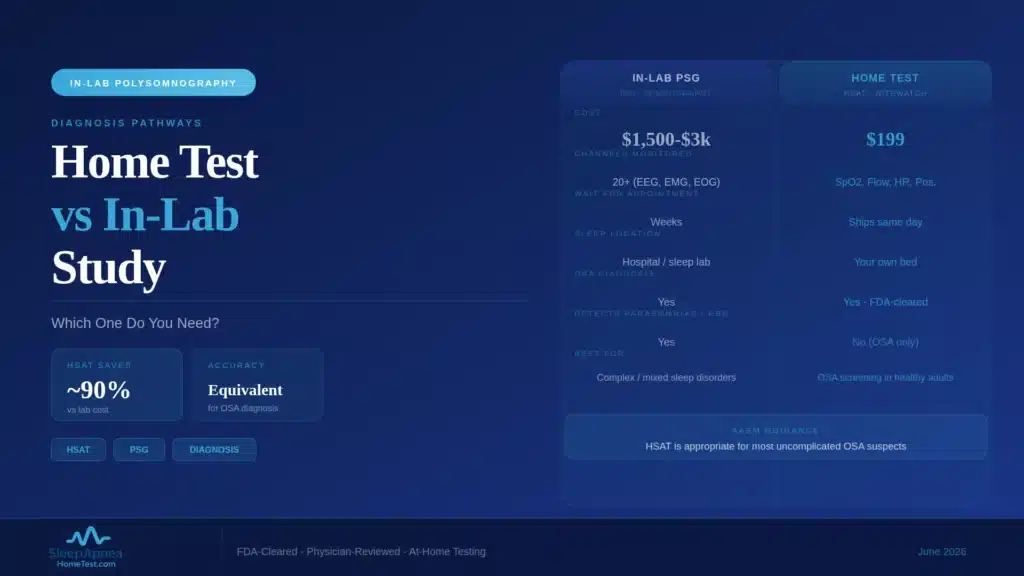
A screening score is a starting point, not an endpoint. If a tool like STOP-BANG or the Epworth scale suggests your daytime tiredness is more than ordinary fatigue, the productive next step is a test that measures what is actually happening while you sleep. For suspected obstructive sleep apnea, that means recording your breathing, oxygen, and pulse overnight.
For most adults without significant heart or lung disease, this does not require a sleep lab. A home sleep apnea test measures your Apnea-Hypopnea Index in your own bed, and a physician reviews the recording and reports the result. If the cause of your tiredness turns out to be something other than apnea, that result still moves the evaluation forward, because ruling apnea out is itself useful information that points a sleep physician toward the next question. The goal is to convert an unexplained symptom into a specific, treatable diagnosis rather than tolerating it indefinitely.
Frequently Asked Questions
Why am I tired even though I sleep 8 hours?
Eight hours in bed is not the same as eight hours of restorative sleep. Conditions like obstructive sleep apnea or periodic limb movements can fragment your sleep into short pieces and rob you of deep and REM stages without your awareness, leaving you sleepy despite adequate time in bed.
What is the difference between sleep quality and sleep duration?
Duration is how long you sleep. Quality is how well-structured and uninterrupted that sleep is, whether you cycle properly through light, deep, and REM stages. You can have normal duration but poor quality if something repeatedly interrupts your sleep architecture, and quality is what determines how rested you feel.
Can sleep apnea make me tired even if I do not snore?
Yes. Snoring is common with obstructive sleep apnea but not universal, and it is more often absent in women. OSA fragments sleep through repeated brief arousals that the sleeper does not remember. Persistent daytime sleepiness without obvious snoring can still be sleep apnea, and a an at-home sleep apnea test can confirm or rule it out.
What is idiopathic hypersomnia?
Idiopathic hypersomnia is a central disorder in which a person sleeps a sufficient or long amount of structurally sound sleep yet remains severely sleepy during the day, often with intense grogginess on waking. It is diagnosed differently from sleep apnea, usually with specialized daytime testing, and is managed by a sleep specialist.
When should I see a doctor about being tired all the time?
See a sleep physician if you consistently get seven to nine hours in bed, keep a regular schedule, and still feel sleepy enough to affect your driving, work, mood, or safety. Reports of snoring or breathing pauses from a bed partner, or dozing off unintentionally during the day, are reasons to seek evaluation sooner.
What is the Epworth Sleepiness Scale?
The Epworth Sleepiness Scale is a brief self-rating questionnaire that asks how likely you are to fall asleep in eight everyday situations. A higher total score indicates excessive daytime sleepiness and suggests your tiredness is more than ordinary fatigue. If your score is elevated, a free sleep apnea risk screening is a quick next step.
Content on SleepApneaHomeTest.com is for educational and screening purposes and does not replace consultation with your own physician. Persistent daytime sleepiness should be evaluated by a qualified medical professional.