By Dr. Joshua Roland, MD, FAASM Former Director, CBT-I Clinic in an Outpatient Substance Rehabilitation Setting
Cognitive Behavioral Therapy for Insomnia is the AASM-recommended first-line treatment. Here is what it is and why so few patients get it.
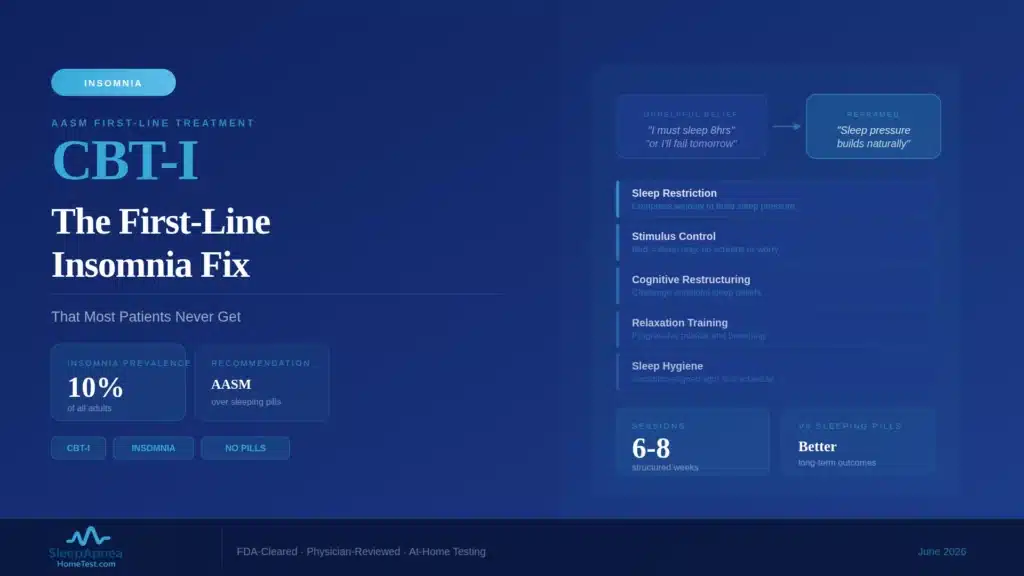
For chronic insomnia, the recommended first-line treatment is not a medication. It is Cognitive Behavioral Therapy for Insomnia, a structured program of roughly 6 to 8 sessions that the American Academy of Sleep Medicine endorses ahead of sleeping pills. It works as well as medication in the short term, works better over the long term, and has no pharmacologic side effects. Yet most people with insomnia are never offered it. Having directed a CBT-I clinic, I want to explain what the treatment is and why the gap between the evidence and everyday practice is so wide.
Quick Facts
- AASM recommendation: CBT-I is first-line treatment for chronic insomnia in adults
- How common insomnia is: chronic insomnia affects roughly 6 to 10 percent of adults
- Typical course: 6 to 8 sessions over roughly 6 to 12 weeks
- Measured effect: CBT-I typically shortens time to fall asleep by 30 to 45 minutes and adds 30 to 60 minutes of total sleep
- Effectiveness: comparable to sleep medication short-term and more durable long-term, with benefits that persist after treatment ends
- The access problem: trained CBT-I providers are in short supply nationally
- Core components: sleep restriction, stimulus control, cognitive therapy, and sleep hygiene
Why CBT-I Is the AASM-Recommended First-Line Treatment
Chronic insomnia is not simply a shortage of sleep. It is a self-sustaining pattern in which difficulty sleeping, anxiety about sleeping, and behaviors meant to compensate, lying in bed longer, napping, watching the clock, all feed each other. Medications can quiet the symptom for a night. They do not dismantle the pattern, and when they stop, the insomnia is usually still there.
CBT-I targets the pattern itself. That is why the American Academy of Sleep Medicine and other major guideline bodies place it ahead of medication for chronic insomnia. The evidence is strong and consistent: across controlled trials, CBT-I typically shortens the time it takes to fall asleep by 30 to 45 minutes and adds 30 to 60 minutes of total sleep, and roughly 36 percent of patients are in remission from insomnia at the end of treatment, compared with about 17 percent in control conditions. CBT-I matches sleeping pills in the short term and outperforms them over months and years, because its effects are learned skills that persist rather than a drug effect that ends with the prescription. It is recommended first not as a gentle alternative but as the more effective treatment.
The Components of CBT-I
CBT-I is not a single technique. It is a small set of evidence-based components delivered together, usually over six to eight sessions.
Sleep restriction is the most powerful and the most counterintuitive. It temporarily limits time in bed to closely match actual sleep time, which consolidates fragmented sleep and rebuilds the natural sleep drive; time in bed is then expanded gradually as sleep solidifies. Stimulus control rebuilds the mental association between bed and sleep, with rules such as using the bed only for sleep and leaving it if you are awake and frustrated. Cognitive therapy addresses the anxious, catastrophic thoughts about sleep that keep the nervous system aroused. Sleep hygiene, the familiar advice about light, caffeine, and routine, is included but is the supporting player, not the core. The first two components do most of the work.
Why Most Patients Get Medications Instead
If CBT-I is more effective, why is it so rarely the treatment people actually receive? The reasons are structural, not clinical. A primary care visit is short, and writing a prescription fits inside it in a way that initiating a multi-week behavioral program does not. Many clinicians were trained when medication was the default and are simply less familiar with CBT-I. Patients often arrive asking for something to help them sleep tonight, and a pill answers that request directly.
There is also a straightforward supply problem, covered in the next section. The combination, time-pressured visits, uneven clinician familiarity, immediate patient expectations, and too few providers, means the path of least resistance is a prescription. None of that reflects the evidence. It reflects how the healthcare system is built. Knowing that the first-line treatment exists is the first step toward asking for it.
The Provider Access Problem and What to Do About It
The single biggest barrier to CBT-I is supply. The number of clinicians formally trained to deliver it is small relative to how common chronic insomnia is, and in many regions there is no in-person CBT-I provider within a reasonable distance. This is a real and well-documented bottleneck.
There are practical ways around it. Many CBT-I therapists now work by telehealth, which erases the geographic limit. Some of the components, particularly sleep restriction and stimulus control, can be guided by a knowledgeable primary care or sleep clinician even without a dedicated CBT-I therapist. And digital CBT-I programs, discussed next, have made the structured protocol far more reachable. If you ask for CBT-I and are told no provider is available locally, telehealth and digital programs are legitimate options to raise.
Digital CBT-I Options and Their Evidence Base
Digital CBT-I delivers the same structured protocol, sleep restriction, stimulus control, cognitive techniques, sleep hygiene, through an app or web program instead of a therapist’s office. The user typically logs a sleep diary, and the program adjusts the prescribed sleep window and delivers the behavioral guidance based on that data.
The evidence for well-designed digital CBT-I is genuinely good. Multiple controlled trials show meaningful improvements in insomnia severity, and several programs have been studied rigorously. Digital CBT-I is not identical to working with a skilled therapist, and people with complex insomnia or significant psychiatric comorbidity are often better served by a clinician. But as a way to deliver an evidence-based first-line treatment to a large number of people who would otherwise get nothing or get a prescription, digital CBT-I is a substantial advance.
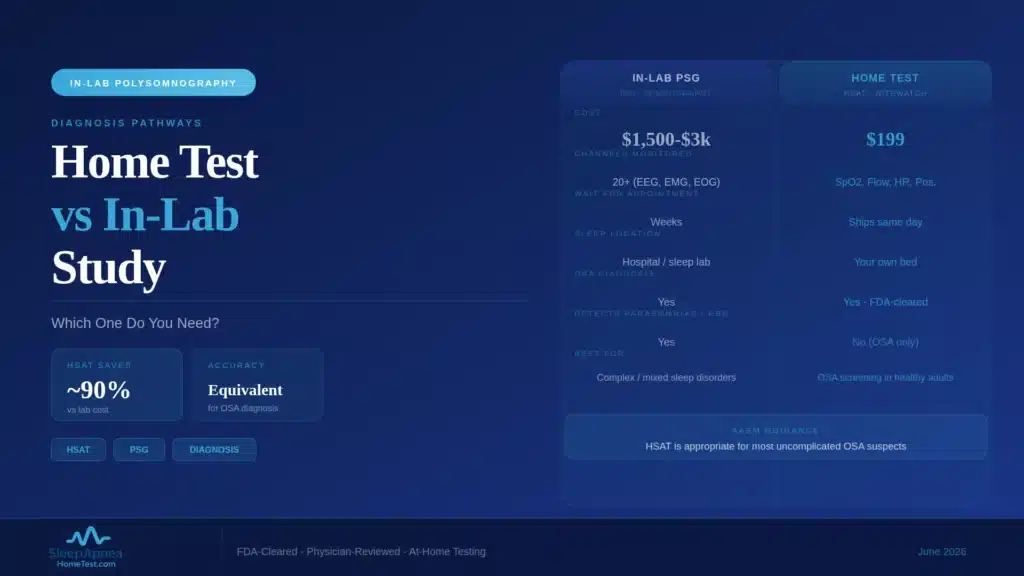
Insomnia and Sleep Apnea: Treatment Sequencing
Insomnia and obstructive sleep apnea overlap more often than many people realize, and when both are present, the order of treatment matters. A patient can have genuine difficulty falling and staying asleep and, underneath it, an undiagnosed breathing disorder fragmenting the sleep they do get.
When the two coexist, treating only one usually disappoints. CBT-I alone may underperform if apnea keeps shredding sleep architecture every night. CPAP alone may be poorly tolerated by someone whose insomnia makes lying in bed with a mask intolerable. The better approach addresses both, often in parallel, with CBT-I for the insomnia pattern and apnea treatment for the breathing. This is also a practical reason to make sure sleep apnea has been ruled in or out before assuming a sleep problem is “just” insomnia. A home sleep apnea test can settle that question without a lab visit.
What I Observed Running a CBT-I Clinic
In directing a CBT-I clinic within an outpatient substance rehabilitation program, a setting where sleep problems are nearly universal and where avoiding sedating medications is a clinical priority, a few things became clear. The first is that patients improve when given the structured protocol, even when their circumstances are difficult and even when they arrived skeptical that anything short of a pill could help.
The second is that the counterintuitive components, especially sleep restriction, require explanation and encouragement, because compressing time in bed feels wrong to someone desperate for sleep, but they are also where the durable gains come from. The third is that CBT-I gives patients a transferable sense of agency over their own sleep, which a prescription does not. None of this is exotic. It is a well-defined treatment that works when it is actually delivered. The problem has never been the treatment. It is access, and access is a problem worth solving.
How to Take the Next Step
If you think you have chronic insomnia, two practical moves make sense. The first is to ask your clinician specifically about CBT-I, by name, and about telehealth or digital options if no in-person provider is available locally. Knowing the treatment exists and asking for it directly is often what changes the conversation from a prescription to a referral.
The second is to make sure a breathing disorder is not hiding underneath the insomnia. Because obstructive sleep apnea and insomnia overlap so often, and because treating the insomnia alone disappoints when apnea is fragmenting sleep every night, it is worth ruling apnea in or out early. A brief sleep apnea risk screening is a low-effort starting point, and if it suggests elevated risk, a home sleep apnea test can settle the question without a lab visit. Addressing both problems together, rather than guessing which one is primary, is the approach most likely to actually restore your sleep.
Frequently Asked Questions
What is CBT-I?
CBT-I, or Cognitive Behavioral Therapy for Insomnia, is a structured, short-term, non-drug treatment for chronic insomnia. Delivered over roughly six to eight sessions, it combines sleep restriction, stimulus control, cognitive therapy, and sleep hygiene to break the self-sustaining pattern that keeps insomnia going.
Is CBT-I better than sleeping pills?
For chronic insomnia, CBT-I matches sleep medication in the short term and outperforms it over the long term. Its benefits are learned skills that persist after treatment ends, whereas medication effects stop when the prescription stops. Major guideline bodies, including the AASM, recommend CBT-I as first-line treatment.
How long does CBT-I take to work?
A typical CBT-I course runs 6 to 8 sessions over about 6 to 12 weeks. Many people notice improvement within the first few weeks, although the sleep-restriction component can briefly feel harder before it helps. The durable benefits build over the full course and persist afterward.
Why did my doctor prescribe medication instead of CBT-I?
This usually reflects system constraints rather than the evidence. Short appointments fit a prescription more easily than starting a multi-week program, some clinicians are less familiar with CBT-I, and trained providers are in short supply. You can ask your clinician specifically about CBT-I, including telehealth and digital options.
Does CBT-I work online or through an app?
Yes. Digital CBT-I programs deliver the same structured protocol through an app or website and have meaningful supporting evidence from controlled trials. Digital programs are not identical to working with a skilled therapist and may not suit complex cases, but they make an evidence-based first-line treatment far more accessible.
Can I have both insomnia and sleep apnea?
Yes, and the overlap is common. Undiagnosed obstructive sleep apnea can fragment sleep beneath an insomnia complaint, and treating only one tends to disappoint. Ruling sleep apnea in or out is a sensible early step; a order an at-home sleep apnea test can settle the question without a lab visit.
How do I find out if sleep apnea is part of my insomnia?
Start with a free sleep apnea risk screening, which gauges your likelihood of obstructive sleep apnea from validated risk factors in a couple of minutes. If your risk is elevated, a physician-reviewed home sleep test measures your Apnea-Hypopnea Index overnight, so the insomnia and any breathing disorder can be addressed together rather than guessed at.
Content on SleepApneaHomeTest.com is for educational purposes and does not replace consultation with your own physician. Chronic insomnia should be evaluated by a qualified medical professional, who can help determine whether CBT-I, treatment of a coexisting condition, or another approach is appropriate.