By Dr. Joshua Roland, MD, FAASM First author, “Impact of Pharmacotherapy on Insomnia in Patients with Alzheimer’s Disease,” Drugs & Aging
Untreated sleep apnea is associated with higher risk of cognitive decline. Here is what the evidence shows and what to do about it.
Untreated obstructive sleep apnea is associated with measurably higher rates of cognitive decline, and large studies have linked it to roughly a 26 percent higher risk of developing dementia or significant cognitive impairment. A growing body of research also suggests that treating sleep apnea may reduce that risk. The relationship runs in both directions: sleep apnea appears to accelerate brain aging, and the diseases of brain aging in turn worsen sleep. Having published peer-reviewed work on sleep and Alzheimer’s disease, I want to walk through what the evidence actually supports, without overstating it.
Quick Facts
- Association: untreated OSA is linked to a roughly 26 percent higher risk of cognitive impairment in pooled cohort studies
- Alzheimer’s-specific risk: a 2025 meta-analysis of 39 cohort studies found a hazard ratio of 1.45 for Alzheimer’s disease in people with OSA
- Proposed mechanisms: intermittent low oxygen, sleep fragmentation, and impaired overnight clearance of brain waste
- Severity matters: higher Apnea-Hypopnea Index correlates with poorer cognitive performance
- Treatment signal: consistent CPAP use is associated with better cognitive outcomes in several studies
- The link is bidirectional: OSA may accelerate cognitive decline, and Alzheimer’s disease worsens sleep
- What the evidence is: largely observational, showing strong association rather than proven causation
The OSA-Cognition Connection
The brain is one of the most oxygen-dependent organs in the body, and it is also where the daily consequences of poor sleep show up first. Obstructive sleep apnea attacks both of those vulnerabilities at once. Every apnea event produces a brief drop in blood oxygen and a brief arousal from sleep, and over a night that can mean hundreds of each.
Researchers studying the OSA-cognition link focus on three plausible pathways. Intermittent hypoxia, the repeated dips in oxygen, produces oxidative stress and inflammation that can damage neurons over time. Sleep fragmentation interrupts the deep and REM stages that consolidate memory. And disrupted sleep appears to impair the brain’s overnight waste-clearance process. None of these is a smoking gun on its own, but together they offer a coherent biological reason why untreated OSA and cognitive decline would be linked.
What the Population Research Finds
The strongest evidence for the OSA-dementia connection comes from large observational studies that follow people over years. A 2025 meta-analysis pooling 39 cohort studies found that obstructive sleep apnea was associated with a hazard ratio of 1.33 for all-cause dementia and 1.45 for Alzheimer’s disease specifically. Put plainly, people with untreated OSA developed dementia at meaningfully higher rates than comparable people without it, even after accounting for age, obesity, and cardiovascular risk factors.
It is important to be precise about what this means. Observational research demonstrates association, not proof of causation. People with OSA differ from people without it in many ways, and statistical adjustment is imperfect. What this research establishes is a consistent, sizable, and biologically plausible link: across dozens of studies and tens of thousands of patients, the direction and rough magnitude hold. It does not establish that OSA single-handedly causes Alzheimer’s disease. That distinction matters, because it shapes how confidently anyone, including a physician, should speak about treatment changing outcomes.
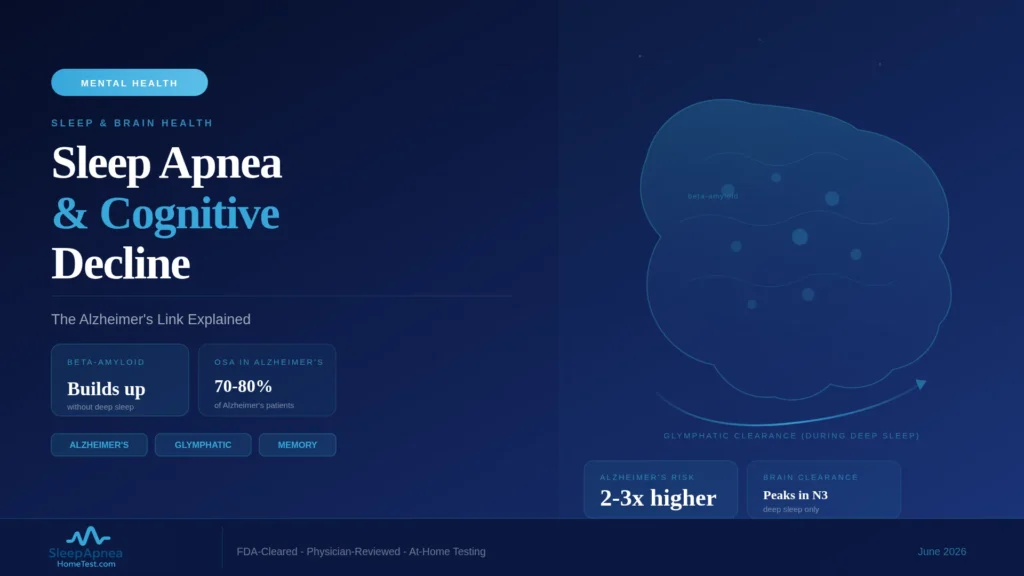
Glymphatic Clearance and Sleep
One of the more compelling threads in this research is the glymphatic system, the brain’s mechanism for flushing metabolic waste. During deep sleep, the spaces between brain cells widen and cerebrospinal fluid moves through brain tissue more freely, carrying away byproducts of daytime activity. Among those byproducts are proteins, including beta-amyloid, that are central to Alzheimer’s disease.
The hypothesis that follows is straightforward: if deep sleep is when the brain clears amyloid, and if obstructive sleep apnea fragments deep sleep night after night, then untreated OSA could allow more amyloid to accumulate over time. This remains an area of active research rather than settled fact, and the human evidence is still developing. But it offers a concrete mechanism linking the nightly disruption of OSA to the slow protein accumulation of Alzheimer’s disease.
CPAP and Cognitive Outcomes
If untreated OSA is associated with cognitive decline, the natural question is whether treatment helps. Several studies suggest it does. In research examining patients who use CPAP consistently, treated OSA is associated with better cognitive performance and, in some studies, slower decline compared with untreated OSA.
The honest summary is that the treatment evidence is encouraging but not yet conclusive. The benefit appears real, appears to depend on consistent use, and appears greater the earlier treatment begins. What the research does not yet show is a guarantee that CPAP prevents dementia. The reasonable position, and the one I take with patients, is that treating sleep apnea is worthwhile on its own substantial merits, daytime function, cardiovascular health, quality of life, and that the cognitive evidence adds a further, serious reason to take diagnosis and treatment seriously.
The Bidirectional Relationship
The link between sleep and cognition is not a one-way street, and this is where my own published work sits. Obstructive sleep apnea may accelerate cognitive decline, but Alzheimer’s disease and related dementias also degrade sleep. As these conditions progress, they disrupt the brain’s sleep-regulating circuitry, producing insomnia, fragmented nights, and disturbed day-night rhythm.
This creates a difficult cycle. Poor sleep may worsen the disease, and the disease worsens sleep. For patients and families managing dementia, sleep disturbance is one of the most distressing symptoms and a frequent reason for caregiver burnout. Recognizing the bidirectional nature of the relationship is important: it means sleep is worth attention both as a possible risk factor earlier in life and as a treatable source of suffering once cognitive disease is established.
What This Means for Screening Older Adults
The practical takeaway is about screening. Obstructive sleep apnea is common in older adults, frequently underdiagnosed, and treatable, and it often presents atypically in this group. Rather than the classic loud snoring, an older adult with OSA may show daytime sleepiness, attention problems, low mood, or what looks like early memory trouble.
That overlap is the reason OSA deserves consideration when an older adult or their family notices new cognitive symptoms. Sleep apnea is not the explanation for every case of memory change, and it is not a substitute for proper neurological evaluation. But it is a genuinely treatable contributor that is easy to overlook, and identifying it can improve daytime function regardless of what else is going on. A home sleep apnea test is an accessible way to evaluate that possibility without a lab visit.
Clinical Recommendations
If I were to distill this into guidance, it would be three points. First, take sleep apnea symptoms seriously at any age, but especially in mid and later life, because the cognitive stakes add to the already strong cardiovascular and quality-of-life reasons for treatment. Second, if an older adult develops new cognitive symptoms, include sleep apnea in the evaluation rather than assuming the cause; it is treatable and easily missed. Third, do not let the dementia research become a source of fear. The evidence supports treating OSA, and treatment carries broad benefits. It does not support the idea that a sleep apnea diagnosis is a sentence of cognitive decline.
What This Means for Families
For families noticing memory or attention changes in an older relative, the practical takeaway is to widen the list of possibilities before settling on a conclusion. Cognitive change is frightening, and it is easy to assume the worst. But several treatable conditions can produce or worsen cognitive symptoms, and untreated obstructive sleep apnea is one of the most common and most reversible of them.
This does not mean a sleep test replaces a proper memory evaluation. It means the two belong in the same workup. If a relative snores heavily, has witnessed breathing pauses, or is persistently sleepy during the day alongside the cognitive changes, raising sleep apnea with their physician is reasonable and constructive. A home sleep apnea test is an accessible way to evaluate that possibility without an overnight lab visit, and it can be arranged in parallel with neurological assessment rather than instead of it.
A Reason to Act Rather Than Worry
The research on sleep apnea and cognition can read as alarming, and that is the wrong takeaway. The constructive reading is that this is a modifiable risk factor sitting within reach. Unlike age or genetics, obstructive sleep apnea can be identified with a simple test and treated effectively, and the cognitive evidence, while not yet conclusive, adds weight to reasons for treatment that were already strong.
If you have symptoms of sleep apnea, the productive response is not worry but a test. A brief risk screening is a low-effort way to gauge whether testing is warranted. Identifying and treating sleep apnea improves daytime function, cardiovascular health, and quality of life regardless of what the long-term cognitive research ultimately confirms, and those benefits are reason enough to act.
Frequently Asked Questions
Does sleep apnea cause Alzheimer’s disease?
The evidence shows a strong, consistent association between untreated obstructive sleep apnea and higher rates of cognitive decline and dementia, but it does not prove that OSA causes Alzheimer’s disease. The research is largely observational. What it establishes is that OSA is a biologically plausible and treatable risk factor worth addressing.
Can treating sleep apnea reduce my risk of dementia?
Several studies associate consistent CPAP use with better cognitive outcomes and slower decline compared with untreated OSA. The benefit appears real and use-dependent, but the evidence does not yet conclusively prove that treatment prevents dementia. Treating sleep apnea is worthwhile for many reasons, and the cognitive evidence adds another.
How does sleep apnea affect the brain?
Obstructive sleep apnea exposes the brain to repeated drops in oxygen, repeated arousals that fragment restorative sleep, and disruption of the deep sleep during which the brain clears metabolic waste, including proteins linked to Alzheimer’s disease. Over years, these effects are thought to contribute to cognitive decline. A an at-home sleep apnea test can measure how severe these events are.
What is the glymphatic system and why does it matter for sleep apnea?
The glymphatic system is the brain’s overnight waste-clearance process, most active during deep sleep, when cerebrospinal fluid flushes byproducts including beta-amyloid from brain tissue. Because obstructive sleep apnea fragments deep sleep, researchers hypothesize that untreated OSA may reduce this clearance over time, allowing more of these proteins to accumulate across years of disrupted nights.
Should an older adult with memory problems be tested for sleep apnea?
Yes, it is worth including. Obstructive sleep apnea is common and underdiagnosed in older adults, often presents as sleepiness or attention and memory trouble rather than snoring, and is treatable. It is not the cause of every memory change and does not replace neurological evaluation, but identifying it can improve daytime function. A free risk screening is a low-effort first step.
Does poor sleep get worse as dementia progresses?
Yes. The relationship is bidirectional. Alzheimer’s disease and related dementias disrupt the brain’s sleep-regulating circuitry, producing insomnia, fragmented sleep, and disturbed day-night rhythm. Sleep disturbance is one of the most distressing symptoms for patients and families, a frequent driver of caregiver burnout, and itself worth treating even when the underlying disease cannot be reversed.
Content on SleepApneaHomeTest.com is for educational purposes and does not replace consultation with your own physician. New or worsening cognitive symptoms should be evaluated by a qualified medical professional; sleep apnea is one treatable factor among others.