By Dr. Joshua Roland, MD, FAASM Co-author, 2023 AASM Clinical Practice Guideline on the Management of REM Sleep Behavior Disorder
What RBD is, what causes it, how it is diagnosed, and the current treatment landscape per the AASM guideline.
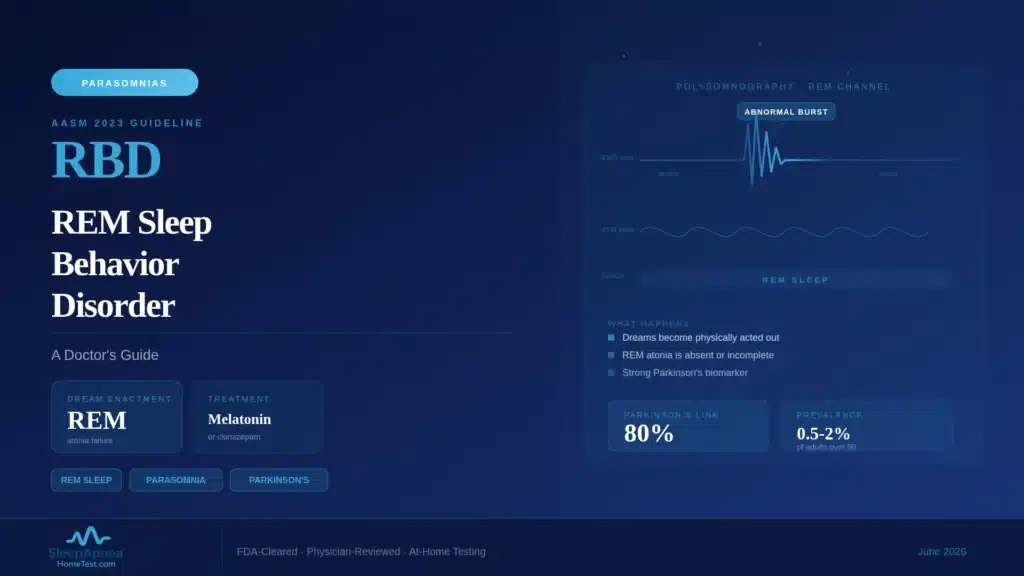
REM sleep behavior disorder is a parasomnia in which the muscle paralysis that normally accompanies REM sleep fails, allowing a sleeper to physically act out vivid, often violent dreams. It is diagnosed with an attended, video-recorded sleep study, and it carries a connection to neurodegenerative disease that makes early recognition genuinely important. As a co-author of the 2023 AASM clinical practice guideline on RBD management, I want to lay out clearly what this condition is and why it deserves attention.
Quick Facts
- What it is: REM sleep without the normal muscle atonia, so dreams are physically enacted
- Core symptom: punching, kicking, shouting, or leaping from bed during vivid dreams
- Typical age of onset: 50 to 65
- Neurodegeneration link: a majority of isolated RBD patients develop an alpha-synucleinopathy, such as Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy, over 10 to 15 years
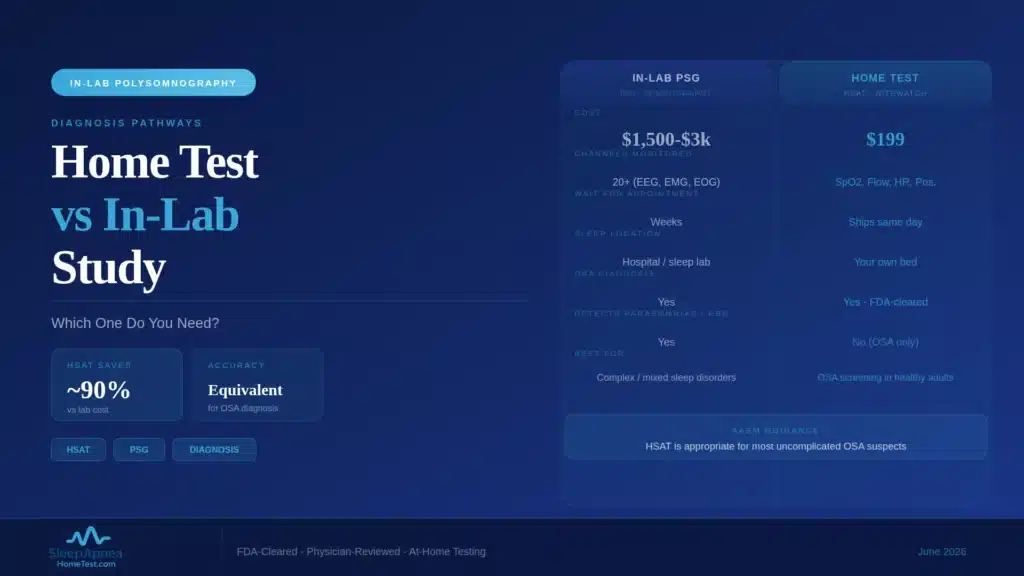
- Diagnosis: requires video-polysomnography; a home sleep apnea test cannot diagnose RBD
- First-line treatment options per the 2023 AASM guideline: melatonin and clonazepam
What RBD Is, and What It Is Not
During normal REM sleep, the stage when most vivid dreaming happens, the body enters a state of near-complete muscle paralysis called atonia. This is protective. It keeps you still while your brain generates dream activity. In REM sleep behavior disorder, that atonia is lost or incomplete, and the body executes the movements of the dream.
This is different from sleepwalking, which arises out of deep non-REM sleep earlier in the night and involves complex but non-dream-driven behavior. It is also different from a nightmare, which is a distressing dream without enacted movement. The hallmark of RBD is the pairing: a vivid, often confrontational dream, and physical behavior that matches it. Partners frequently describe being struck or kicked, and injuries to the sleeper or bed partner are common reasons people finally seek evaluation.
The 2023 AASM Clinical Practice Guideline
In 2023, the American Academy of Sleep Medicine published an updated clinical practice guideline on the management of REM sleep behavior disorder, alongside a companion systematic review, meta-analysis, and GRADE assessment. I served on the task force that produced this work. The guideline is the reference document sleep physicians use when managing RBD, and it is the basis for the treatment section below.
The guideline’s central contributions are a structured assessment of the available treatment evidence and clear, evidence-graded recommendations. It also formalizes the link between isolated RBD and later neurodegeneration, which shapes how clinicians counsel patients after diagnosis. When this article describes “first-line” treatment, it is referencing the guideline’s graded recommendations, not informal practice.
Why a Home Sleep Test Cannot Diagnose RBD
This is a point worth stating plainly. A home sleep apnea test cannot diagnose REM sleep behavior disorder. Diagnosing RBD requires video-polysomnography, an attended in-lab study that records brain-wave activity, eye movement, and chin and limb muscle tone, with synchronized video of the patient.
Two of those signals are essential and absent from a home test. The brain-wave and eye-movement channels are what confirm that an event occurred specifically during REM sleep. The chin-muscle channel is what documents the loss of REM atonia, the defining physiological finding. The synchronized video lets the physician see the behavior and match it to the sleep stage. A home test, built to count breathing events, captures none of this. If RBD is suspected, the correct path is referral to a sleep center for video-PSG.
The Neurodegeneration Connection
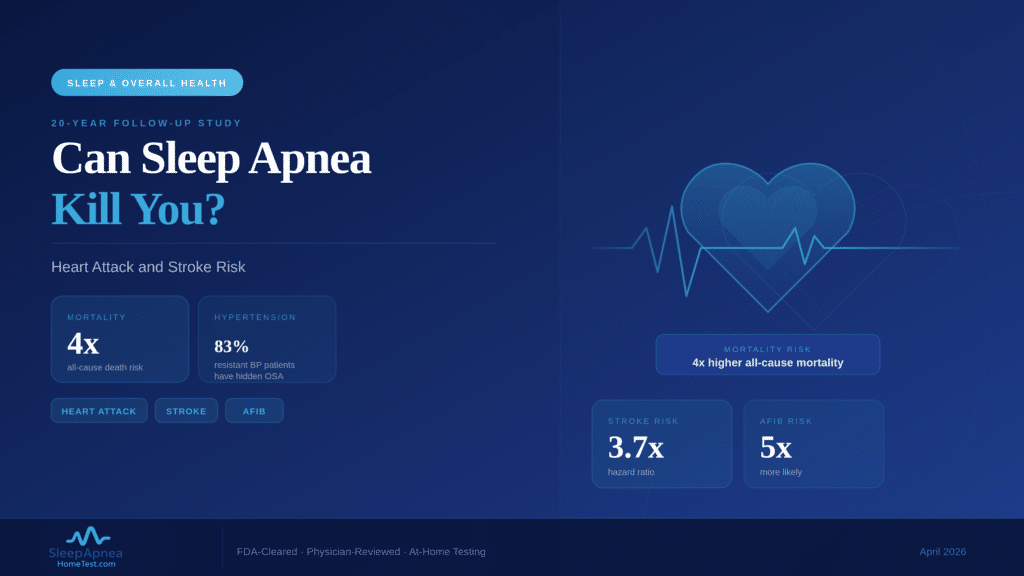
The most important fact about isolated RBD is its relationship to neurodegenerative disease. Long-term follow-up research finds that a substantial majority of people diagnosed with isolated RBD, meaning RBD without another known cause, go on to develop an alpha-synucleinopathy over the following 10 to 15 years. That category includes Parkinson’s disease, dementia with Lewy bodies, and multiple system atrophy.
This sounds alarming, and the counseling around it requires care, which is part of why diagnosis belongs with a sleep physician. But the connection is also an opportunity. RBD is one of the earliest detectable signals of these conditions, sometimes preceding motor symptoms by a decade or more. That long lead time is exactly the window that neuroprotective research is trying to use. A diagnosis of RBD is a reason for structured neurological follow-up, not a verdict.
Treatment Options and the Evidence Base
Treatment of RBD has two goals: reduce injury and improve sleep safety. The first and often most effective step is environmental. Padding sharp furniture corners, lowering the mattress or using a floor mattress, removing bedside objects, and at times a bed partner sleeping separately all reduce injury risk immediately, independent of medication.
For pharmacologic treatment, the 2023 AASM guideline evaluates the available options and their evidence. Melatonin and clonazepam are the most established treatments and are used first-line, with the choice between them shaped by each patient’s other conditions, age, and risk profile. Clonazepam can cause daytime sedation and is used cautiously in older adults and in anyone with concurrent obstructive sleep apnea or cognitive impairment. Melatonin has a more favorable side-effect profile for many patients. Treatment is individualized, and that is genuinely a conversation to have with a sleep physician rather than a decision to make from an article.
RBD Versus Other Parasomnias
Because the behaviors can look similar from the outside, RBD is often confused with other parasomnias, and the distinction matters because the workup and the implications differ. Sleepwalking and night terrors are non-REM parasomnias. They emerge from deep slow-wave sleep, usually in the first third of the night, are more common in children, and do not carry the neurodegeneration association.
RBD, by contrast, emerges from REM sleep, usually in the second half of the night when REM is concentrated, typically begins after age 50, and is dream-enactment behavior specifically. Sleep talking can occur in any stage and is generally benign. When a physician hears “acting out dreams in a 60-year-old,” RBD moves to the top of the list, and that is what prompts referral for video-PSG.
Where RBD Sits Among Sleep Disorders
It helps to place RBD in the wider landscape of sleep medicine, because patients often arrive worried they have one condition when the history points to another. RBD is a parasomnia, a category of abnormal behavior during sleep, and it is distinct from the sleep-disordered breathing conditions that account for most sleep referrals. Obstructive sleep apnea, the most common of those, is a breathing problem and is screened for very differently. If breathing pauses or loud snoring are the main complaint, a home sleep apnea test is the appropriate first step, not video-PSG.
The two can coexist, and that overlap matters for treatment. A patient may have both RBD and obstructive sleep apnea, and untreated apnea can fragment sleep in ways that complicate the clinical picture. It is also worth knowing that some apnea events produce movement and vocalization that a bed partner mistakes for dream enactment. This is one more reason the diagnosis belongs in a sleep lab: video-PSG can distinguish a genuine REM-sleep parasomnia from arousals driven by a breathing disorder. If you are unsure which problem you are dealing with, a brief sleep apnea risk screening is a reasonable way to begin sorting it out before a specialist visit.
What Happens After an RBD Diagnosis
A diagnosis of RBD sets several things in motion beyond the prescription pad. The first is safety, addressed through the environmental measures described below and reviewed at follow-up visits. The second is treatment of the behavior itself, individualized to the patient. The third, and the one patients should expect, is a plan for neurological follow-up.
Because isolated RBD is an early marker of alpha-synucleinopathy, sleep physicians typically arrange periodic neurological assessment, watching for the subtle motor, cognitive, or autonomic changes that can precede a formal Parkinson’s or related diagnosis. This is not a cause for alarm; it is the appropriate use of a long lead time. Catching those changes early opens the door to earlier symptom management and, increasingly, to research participation. The follow-up plan is part of what makes a proper diagnosis valuable rather than merely a label. To understand how sleep apnea fits into the same neurodegeneration picture, see our related article on sleep apnea and Parkinson’s risk.
When to See a Sleep Medicine Physician
You should seek evaluation if you or a bed partner notice repeated dream-enactment behavior: punching, kicking, shouting, or leaping from bed in apparent response to a dream. The threshold is lower if there has been an injury, if the behavior is escalating, or if it began after age 50.
A sleep medicine physician will take a detailed history, often interview the bed partner, and arrange video-polysomnography if RBD is suspected. Diagnosis matters not only for treating the behavior and preventing injury but for establishing the neurological follow-up that the diagnosis warrants. RBD is a manageable condition, and it is also a meaningful early signal. Both of those are reasons to take it to a specialist rather than wait.
Frequently Asked Questions
What is the difference between RBD and sleepwalking?
RBD arises from REM sleep, usually in the second half of the night, and involves enacting vivid dreams; it typically begins after age 50. Sleepwalking arises from deep non-REM sleep early in the night, is more common in children, and is not dream-driven. RBD also carries a neurodegeneration link that sleepwalking does not.
Can a home sleep apnea test detect REM sleep behavior disorder?
No. Diagnosing RBD requires video-polysomnography in a sleep lab, which records brain-wave activity, eye movement, chin-muscle tone, and synchronized video. A home sleep apnea test measures breathing and oxygen only, so it cannot confirm that behavior occurred during REM sleep or document the loss of REM muscle atonia. A home sleep apnea test is the right tool for suspected obstructive sleep apnea, not RBD.
Does having RBD mean I will get Parkinson’s disease?
Not certainly, but the risk is significant. Long-term follow-up research finds that a majority of people with isolated RBD develop an alpha-synucleinopathy, such as Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy, over 10 to 15 years. A diagnosis of RBD is a reason for structured neurological follow-up so that any changes are caught early.
How is REM sleep behavior disorder treated?
Treatment starts with making the sleep environment safe: padding furniture, lowering the bed, and removing hazards. The 2023 AASM guideline identifies melatonin and clonazepam as established first-line medications, with the choice individualized by age and other conditions. Treatment should be directed by a sleep medicine physician.
At what age does RBD usually start?
Isolated REM sleep behavior disorder most often begins between ages 50 and 65 and is more common in men, though it occurs in women as well. RBD can also appear at younger ages when it is associated with narcolepsy or with certain medications, particularly some antidepressants.
Is RBD dangerous?
The main immediate danger is injury. Because the sleeper physically enacts dreams, falls, punches, and collisions with furniture or a bed partner are common, and injuries are a frequent reason people seek care. Making the bedroom safe addresses that risk directly. The longer-term significance is the neurodegeneration link, which calls for follow-up rather than alarm.
Should I see a doctor if my partner acts out dreams?
Yes. Repeated dream-enactment behavior, especially in someone over 50 or when an injury has occurred, warrants evaluation by a sleep medicine physician. The behavior is treatable, and diagnosis also establishes the neurological monitoring an RBD diagnosis warrants. If breathing pauses or snoring are also part of the picture, a free sleep apnea risk screening can help sort out what is driving the night-time activity.
Content on SleepApneaHomeTest.com is for educational purposes and does not replace consultation with your own physician. REM sleep behavior disorder is diagnosed and managed by sleep medicine physicians through in-lab video-polysomnography; it cannot be diagnosed with a home sleep apnea test.