By Dr. Joshua Roland, MD, FAASM Co-author, “Obesity Hypoventilation Syndrome” chapter in Clinics in Chest Medicine
OHS is sleep-disordered breathing plus daytime hypoventilation. Here is how to recognize it, why it is often missed, and how it is treated.
Obesity hypoventilation syndrome is defined by three things together: obesity, with a body mass index of 30 or higher; chronic daytime hypoventilation, meaning elevated carbon dioxide in the blood that persists while awake; and the absence of another condition that would explain it. Most people with OHS also have obstructive sleep apnea, which is exactly why OHS is so often missed. It hides behind an OSA diagnosis. Having co-authored the reference chapter on this condition, I want to make the distinction clear, because the treatment and the stakes are different.
Quick Facts
- What it is: BMI of 30 or higher plus chronic daytime hypercapnia, arterial CO2 of 45 mmHg or higher, with no other cause
- Prevalence: roughly 10 to 20 percent of obese patients evaluated for obstructive sleep apnea
- Mortality if untreated: meaningfully higher than OSA alone
- Why it is missed: frequently diagnosed as OSA without the arterial blood gas testing that would reveal hypoventilation
- Typical treatment: weight management, positive airway pressure therapy, often BiPAP rather than CPAP, and supplemental oxygen when needed
OHS Versus OSA: The Critical Distinction
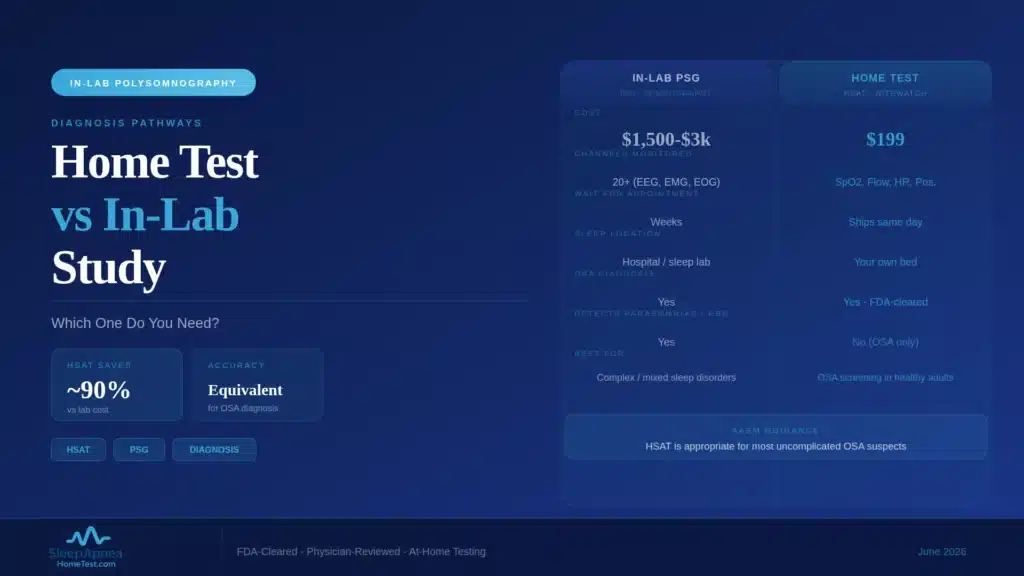
Obstructive sleep apnea is a problem of the airway. The throat collapses repeatedly during sleep, breathing pauses, oxygen dips, and the sleeper briefly wakes to reopen the airway. Between events, an OSA patient breathes normally and clears carbon dioxide normally. Their daytime blood gases are usually fine.
Obesity hypoventilation syndrome is a problem of ventilation itself. The work of moving air is increased by body habitus, the drive to breathe is blunted, and the result is that carbon dioxide is not fully cleared, not just at night but around the clock. The defining feature is daytime hypercapnia: elevated CO2 measured while the patient is awake. A person can have OSA without OHS. A person with OHS usually also has OSA. The two travel together, and that overlap is the source of most missed diagnoses.
Why Home Sleep Apnea Testing Alone Misses OHS
A home sleep apnea test is built to do one job well: detect obstructive sleep apnea by measuring airflow, effort, oxygen, and pulse overnight. It does that job accurately for uncomplicated OSA. What it cannot do is measure daytime carbon dioxide.
Hypoventilation in OHS is confirmed by an arterial blood gas, a daytime blood draw analyzed for CO2, or by a daytime venous CO2 or a serum bicarbonate that hints at chronic retention. None of that is part of a home sleep study. So a patient with OHS can complete a home test, receive an accurate OSA diagnosis, start CPAP, and still have the hypoventilation component entirely undetected. The home test was not wrong. It simply answered a narrower question than the patient’s situation required. This is the central reason a thorough physician keeps OHS in mind for any patient who is both obese and short of breath.
The Diagnostic Workup
Diagnosing OHS requires going beyond the sleep study. When OHS is suspected, the workup adds an arterial blood gas to document daytime hypercapnia, which is the finding that confirms the diagnosis. A serum bicarbonate is often checked first as an inexpensive screen; a normal bicarbonate makes significant chronic hypercapnia less likely.
Pulmonary function tests help rule out other causes of elevated CO2, such as severe COPD, so the “no other explanation” part of the definition is satisfied. An in-lab sleep study is frequently used as well, because it can measure CO2 through the night and characterize the breathing pattern in detail. The point is that OHS is not diagnosed by a single test. It is diagnosed by recognizing the pattern, an obese patient with daytime hypercapnia, and confirming it deliberately.
Treatment: Weight, PAP, and Oxygen
Treatment of OHS works on the underlying problem rather than only the nighttime events. Weight management is foundational, because the condition is driven by body habitus, and meaningful weight reduction can improve or even resolve the hypoventilation over time.
Positive airway pressure is the mainstay for the breathing itself. Many OHS patients are treated with bilevel PAP, often called BiPAP, rather than the fixed CPAP used for straightforward OSA, because bilevel support actively assists ventilation and helps clear carbon dioxide. Some patients also need supplemental oxygen, particularly early in treatment. The treatment plan is individualized and managed by a physician, frequently a pulmonologist or sleep specialist, because the device choice and the oxygen decision depend on the specific blood-gas picture.
Cardiovascular and Metabolic Comorbidity
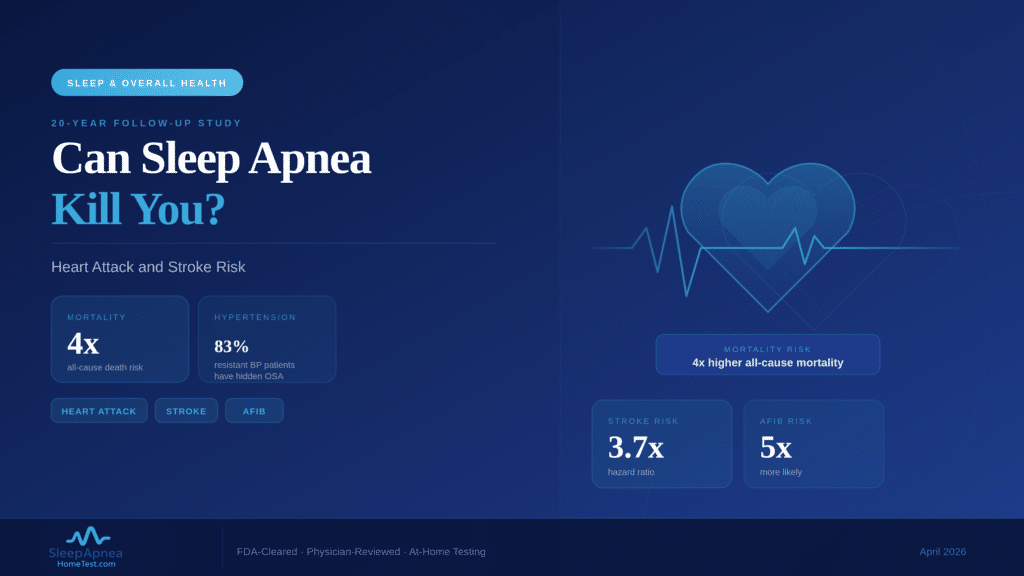
OHS rarely travels alone. Patients with obesity hypoventilation syndrome carry a heavy burden of cardiovascular and metabolic disease: hypertension, heart failure, pulmonary hypertension, type 2 diabetes, and metabolic syndrome are all common companions. Pulmonary hypertension in particular is more frequent and more severe in OHS than in OSA alone.
This clustering is part of why untreated OHS carries higher mortality than OSA by itself. The chronic strain of inadequate ventilation, combined with the comorbid load, accelerates cardiovascular decline. It is also why diagnosing OHS changes management beyond the sleep apnea: it prompts closer attention to the heart, the lungs, and metabolic health together.
Long-Term Outcomes With Proper Treatment
The encouraging part of the picture is that OHS responds to treatment. With consistent positive airway pressure therapy, weight management, and treatment of the comorbid conditions, patients see improved daytime carbon dioxide levels, better daytime alertness, fewer hospitalizations, and improved survival compared with untreated disease.
The barrier is recognition. Because OHS so often sits hidden behind an OSA diagnosis, the patients who do worst are usually the ones whose hypoventilation was never identified. Once it is named and treated, the trajectory changes substantially. That is the practical case for keeping OHS in mind.
How OHS Changes the Treatment of Sleep Apnea
For a patient who has both obstructive sleep apnea and obesity hypoventilation syndrome, recognizing the OHS component changes the treatment plan in concrete ways. Straightforward OSA is often treated with fixed-pressure CPAP. OHS frequently calls for bilevel PAP instead, because the two pressure levels actively assist ventilation and help clear the retained carbon dioxide that fixed CPAP alone may not address. Choosing the wrong device is a common reason a patient feels no better despite using their machine faithfully.
The monitoring also differs. An OSA patient’s progress can often be tracked through symptoms and device data. An OHS patient needs periodic checks of daytime carbon dioxide to confirm the hypoventilation is actually improving, not just the nighttime apnea events. This is why the distinction is not academic. A patient diagnosed with sleep apnea through a home sleep test who also fits the OHS profile should have that second question asked deliberately, because it determines which machine they are sent home with and how their recovery is measured.
Why Early Identification Matters
OHS tends to be diagnosed late, often only after a patient is hospitalized with respiratory failure. By that point the cardiovascular and pulmonary strain has accumulated for years. Earlier identification, ideally when a patient is first evaluated for sleep apnea rather than after a crisis, allows treatment to begin before pulmonary hypertension and right-heart strain are advanced.
The practical message for patients is to take breathlessness seriously and to be specific with clinicians about it. If you are significantly overweight, have been told you have sleep apnea, and are short of breath during the day, that combination is worth raising directly. A simple sleep apnea risk screening can start the conversation, with the clear understanding that a physician should layer in arterial blood gas testing if the OHS pattern is present.
When to Advocate for Testing Beyond a Home Sleep Study
If you are significantly overweight and have been diagnosed with sleep apnea, there are specific symptoms that should prompt a conversation with your physician about testing for hypoventilation. Daytime shortness of breath, morning headaches, swelling in the legs, a bluish tint to the lips or fingertips, and excessive sleepiness that does not improve with CPAP are all signals worth raising.
A home sleep apnea test is a reasonable and accessible way to identify obstructive sleep apnea, and for many people that is the whole story. But if you fit the OHS risk profile, obese and breathless, ask specifically whether your daytime carbon dioxide has been checked. If you have not yet been evaluated for sleep apnea at all, a home sleep test is a sound first step, with the understanding that a physician should layer in additional testing if the OHS pattern is present.
Frequently Asked Questions
What is the difference between OHS and sleep apnea?
Obstructive sleep apnea is repeated airway collapse during sleep, with normal daytime breathing. Obesity hypoventilation syndrome is chronic under-breathing that elevates carbon dioxide around the clock, including while awake. Most people with OHS also have OSA, but OHS adds a daytime ventilation problem that OSA alone does not.
Why does a home sleep test miss obesity hypoventilation syndrome?
A home sleep apnea test measures airflow, effort, oxygen, and pulse overnight. It cannot measure daytime carbon dioxide, which is the finding that defines OHS. A patient with OHS can get an accurate OSA result from a home test while the hypoventilation goes undetected, so additional daytime testing is needed.
How is OHS diagnosed?
OHS is diagnosed by documenting daytime hypercapnia, usually with an arterial blood gas, in a person with a BMI of 30 or higher, after other causes are excluded. A serum bicarbonate is often used as an initial screen, and pulmonary function tests and an in-lab sleep study help complete the picture.
Can OHS be treated?
Yes. Treatment combines weight management, positive airway pressure therapy, often bilevel PAP rather than CPAP, and supplemental oxygen when needed. With consistent treatment, daytime carbon dioxide improves, alertness returns, hospitalizations fall, and survival improves compared with untreated OHS. The first step is identifying it, which begins with evaluating the sleep apnea component through order an at-home sleep apnea test.
Is OHS more dangerous than sleep apnea?
Untreated OHS carries higher mortality than obstructive sleep apnea alone. It clusters with hypertension, heart failure, pulmonary hypertension, and metabolic disease, and the chronic strain of inadequate ventilation accelerates cardiovascular decline. Recognizing and treating it changes that trajectory, which is why the OHS component should be looked for deliberately rather than left hidden behind an OSA diagnosis.
What symptoms suggest I should be tested for OHS rather than just OSA?
Daytime shortness of breath, morning headaches, leg swelling, a bluish tint to the lips or fingertips, and sleepiness that does not improve with CPAP are signals worth raising with your physician, especially if you are significantly overweight. A free sleep apnea risk screening is a starting point; ask specifically whether your daytime carbon dioxide level has been checked.
Content on SleepApneaHomeTest.com is for educational purposes and does not replace consultation with your own physician. Obesity hypoventilation syndrome is diagnosed and managed by physicians through testing that extends beyond a home sleep apnea study.